Artificial intelligence (AI) is rapidly transforming many aspects of healthcare, and radiation oncology has been among the earliest fields to adopt its potential. With its interdisciplinary foundation in clinical oncology, computational sciences, imaging, and physics, radiation oncology is ideally positioned to integrate AI solutions into clinical workflows. Current clinical AI solutions focus on automation tasks in the radiotherapy workflow: Deep learning-based auto-contouring of tumors and organs at risk, automated treatment planning, and dose prediction enable faster and more consistent treatment planning but also facilitate adaptive radiotherapy. The management of inter- and intrafraction anatomical changes, jointly with MR-only workflows, rely strongly on AI-facilitated automation and image-processing methods. Beyond workflow automation, AI is also driving progress toward biology-tailored radiotherapy, aiming for personalization of dose prescription, spatial dose distribution, and treatment schedules. Multimodal concepts in mechanistic and data-driven modelling integrate imaging, genomics, pathology, and clinical data to predict tumor response and toxicity. At the same time, agent-based AI systems powered by large language models (LLMs) are emerging as interactive tools that may extend beyond report automation and trial identification toward supervised clinical decision support. Despite these advances, biology-adaptive radiotherapy remains constrained by limited access to large, high-quality multimodal datasets, challenges in generalizability, and the need for robust AI-specific quality-assurance frameworks. Future progress will depend on trustworthy, human-centered AI systems that augment clinical expertise and support safer, more adaptive, and more personalized radiation oncology.
Künstliche Intelligenz (KI) verändert viele Bereiche des Gesundheitswesens rasant, und die Strahlentherapie gehört zu den ersten Fachgebieten, die ihr Potenzial nutzen. Mit ihrer interdisziplinären Grundlage in den Bereichen klinische Onkologie, Computerwissenschaften, Bildgebung und Physik ist die Strahlentherapie ideal positioniert, um KI-Lösungen in klinische Arbeitsabläufe zu integrieren. Aktuelle klinische KI-Lösungen konzentrieren sich auf Automatisierungsaufgaben im Strahlentherapie-Workflow: Deep-Learning-basierte automatische Konturierung von Tumoren und Risikoorganen, automatisierte Behandlungsplanung und Dosisvorhersage ermöglichen eine schnellere und konsistentere Behandlungsplanung, erleichtern aber auch die adaptive Strahlentherapie. Das Management von anatomischen Veränderungen zwischen und innerhalb von Fraktionen stützt sich, gemeinsam mit reinen MR-Workflows, stark auf KI-gestützte Automatisierung und Bildverarbeitungsmethoden. Über die Automatisierung von Arbeitsabläufen hinaus treibt KI auch den Fortschritt in Richtung einer biologisch massgeschneiderten Strahlentherapie voran, mit dem Ziel der Personalisierung von Dosisverschreibung, räumlicher Dosisverteilung und Behandlungsplänen. Multimodale Konzepte in der mechanistischen und datengesteuerten Modellierung integrieren Bildgebungs-, Genomik-, Pathologie- und klinische Daten, um das Ansprechen des Tumors und die Toxizität vorherzusagen. Gleichzeitig entwickeln sich agentenbasierte KI-Systeme, die auf grossen Sprachmodellen (LLMs) basieren, zu interaktiven Werkzeugen, die über die Automatisierung von Berichten und die Identifizierung von Studien hinausgehen und bis hin zur überwachten klinischen Entscheidungsunterstützung reichen können. Trotz dieser Fortschritte wird die biologisch adaptive Strahlentherapie weiterhin durch den begrenzten Zugang zu grossen, hochwertigen multimodalen Datensätzen, Herausforderungen bei der Verallgemeinerbarkeit und den Bedarf an robusten KI-spezifischen Qualitätssicherungsrahmen eingeschränkt. Zukünftige Fortschritte werden von vertrauenswürdigen, menschenzentrierten KI-Systemen abhängen, die klinisches Fachwissen ergänzen und eine sicherere, anpassungsfähigere und personalisiertere Strahlentherapie ermöglichen.
Keywords: Artificial intelligence, radiation oncology, adaptive radiotherapy, personalized treatment
Introduction
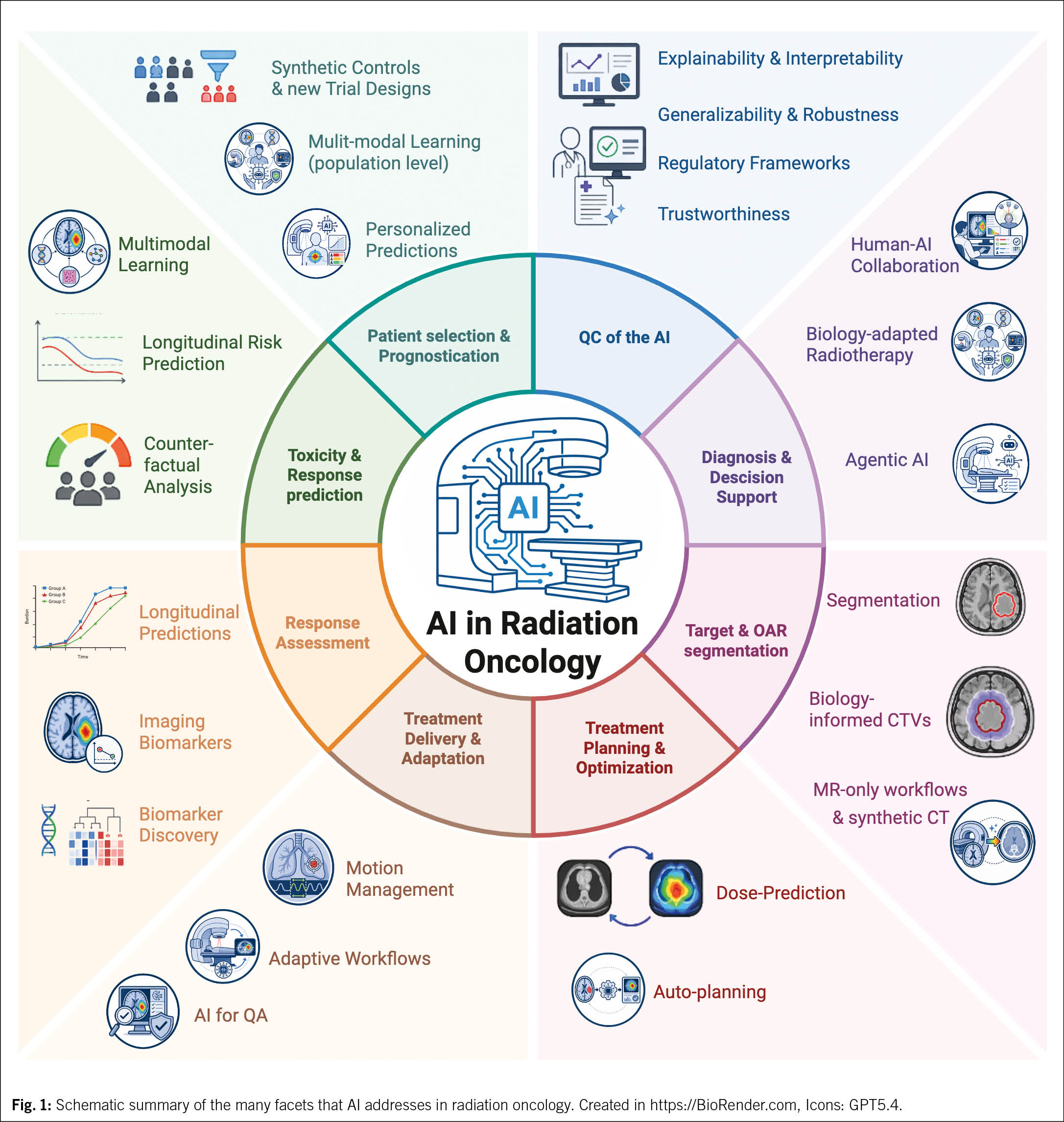
Under the umbrella of artificial intelligence (AI), a range of computational approaches has emerged that differ in method and scope. Many contemporary AI methods, particularly machine learning and deep learning, are characterized by their ability to learn patterns from data, while more recent generative AI systems extend this capability to the creation of new content. Supported by growing digital data resources, advances in computational power, and increasingly powerful model architectures, AI plays an increasing role in the advancement of medicine, transforming diagnostics, treatment, and care delivery at an unprecedented pace (1–3). Radiation oncology was among the first medical disciplines in which AI had a direct impact on clinical workflows and patient outcomes. Owing to its inherent interdisciplinarity, encompassing clinical sciences, medical physics, imaging, and molecular biology, radiation oncology offers numerous opportunities for support through AI (3, 4) as outlined in (Fig. 1).
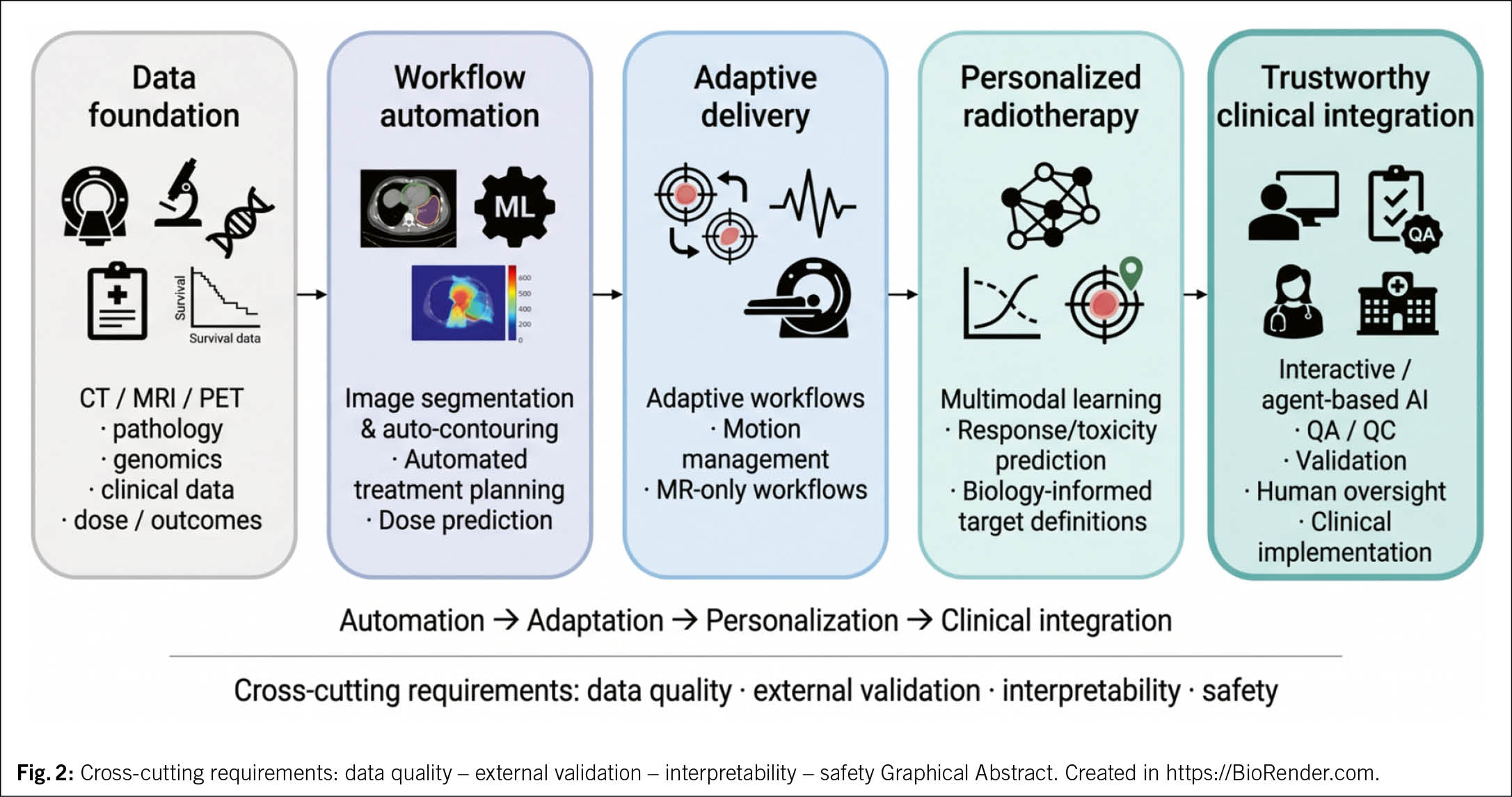
At the same time, the role of AI in radiation oncology can no longer be captured by isolated technical examples alone. The field now includes a broad range of approaches that differ not only in computational methodology, but also in clinical purpose, maturity, and degree of integration into routine care. What was initially judged mainly by algorithmic performance on individual tasks has developed into a broader question of how AI may change radiotherapy workflows, support the use of increasingly heterogeneous data, and redefine the balance between automation-supported efficiency gains and clinical oversight (Fig. 2).
This motivates a more integrated view that covers the diverse application objectives of data-driven solutions in radiation oncology to address models in clinical practice, approaches that remain largely translational, and emerging concepts that may shape the next phase of development. At the same time, the growing scope of AI brings equally important questions about validation, robustness, implementation, trustworthiness, and whether technical progress can be translated into meaningful clinical benefit. Here, we first discuss AI applications that support automation in the radiotherapy workflow, including planning and treatment delivery. We then examine emerging approaches aimed at biology-informed personalization. Finally, we address interactive and agent-based AI systems, as well as the quality assurance and translational challenges that will define their future role in clinical practice.
AI for automation in radiation oncology
Automation of manual steps in the radiotherapy process is one of the main assets of AI. In recent years, the number of publications on this topic has grown steadily, providing increasing evidence of the clinical value of AI-based automation (2, 4). This increasing evidence has also led to commercial tools that comply with regulatory requirements and can be used in clinical practice. More recently, the field has moved beyond proof-of-concept performance studies toward implementation-focused work addressing clinical acceptability, time saving, dosimetric impact, external validation, and performance monitoring in routine use (5–7).
Auto-contouring
Image segmentation (contouring) AI plays a pivotal role in modern radiotherapy by enabling precise delineation of tumors and surrounding organs at risk. Auto-contouring models, particularly variations of convolutional neural networks (CNNs) and U-Net-derived architectures, can be trained on annotated medical images to automatically identify and segment anatomical structures in CT, MRI, or PET scans (8–10). These annotations of anatomical structures are readily available in radiation oncology since they are made routinely in clinical practice for treatment planning and stored in clinical databases.
While to date, a total of 50 commercial auto-contouring tools have been launched (https://dlinrt.eu/dashboard, April 2026), the majority of these approaches address organ-at-risk contouring which benefits from consistent anatomies and image representation that enable high-quality agreement in manual annotations that serve as training data to AI solutions. In contrast, target segmentation still remains more challenging and continues to be an active topic of scientific research (5, 6, 11) with fewer commercial solutions to date. Gross tumor volume segmentation and, in particular, the definition of clinical target volumes (CTVs) may still be subject to larger inter-observer variability stemming from variations in shape, position, imaging appearance, and biological behavior. This makes it more difficult and data-intensive to train broadly acceptable and generalizable target autosegmentations required for multi-institutional rollout. Despite these hurdles, once clinically applied, automation can significantly reduce the time and inter-observer variability associated with manual contouring, ultimately supporting more consistent and efficient treatment planning (5, 6, 11) and adaptive radiotherapy by facilitating rapid re-contouring in response to anatomical changes over the course of treatment (9, 12, 13).
Recent work has also emphasized that the evaluation of auto-segmentation should not rely on geometric metrics alone. Time to correction, expert acceptability, dosimetric consequences, and multicenter robustness are increasingly recognized as clinically relevant endpoints (6, 7, 14). This is particularly important as clinical deployment expands, as even apparently mature OAR applications require local validation and ongoing monitoring before routine use (7, 14, 15).
Automated treatment planning and dose prediction
Planning radiotherapy treatments has traditionally been a time-consuming process, requiring experts to iteratively adjust optimization objectives to obtain dose distributions that balance tumor control and sparing of proximal healthy structures. AI is now accelerating this process through two related approaches: automated treatment planning and dose prediction (16–18).
Automated treatment planning (ATP) uses AI models trained on large-scale retrospective treatment plans, often in combination with established optimization engines, to generate clinically acceptable dose distributions with little or no manual adjustment (16, 17, 19). These systems can substantially reduce planning time while maintaining, and in some settings improving, plan quality. When combined with automated contouring and daily imaging, auto-planning also sets the basis for adaptive workflows accounting for patient anatomy of the day, ultimately supporting dose conformity and improving outcomes (16, 19).
Dose prediction complements ATP by focusing on directly generating high-quality spatial dose distributions (17, 18, 20) thereby offering a rapid prediction of what an optimal or achievable plan may look like based on imaging, tumor location, and clinical prescriptions. While many predicted dose distributions to date may not inherently be also deliverable, dose prediction can be used to benchmark whether a given plan is realistic, can guide planning toward improved organ sparing, and may support plan review and expected treatment outcomes. Increasingly, research and clinical systems are beginning to merge dose prediction with auto-planning, reflecting how these tools are moving into clinical use (17, 18, 20). More recent work has broadened this area toward image enhancement and synthetic image generation in support of planning, including CBCT-to-CT translation, denoising, and synthetic CT generation for dose calculation (13, 21, 22). These developments connect automated planning more closely with treatment delivery. However, important challenges remain, including generalizability across institutions and treatment protocols, transparency of black-box models, and the need to ensure that AI-generated plans are clinically deliverable and not only dosimetrically plausible (3, 15, 18).
AI to support radiotherapy delivery
Beyond treatment planning, the delivery of radiation therapy can also benefit from automation through real-time adaptation and integration into adaptive radiotherapy (ART) workflows to account for anatomical changes (9, 13). These methods emphasize both inter-fraction and intra-fraction precision, leveraging imaging, image synthesis, and motion modeling to improve safety and tumor coverage to effectively shorten the process from image acquisition to treatment plan based on the current anatomy.
Adaptive workflows
ART workflows heavily rely on automating and accelerating several time-consuming and complex tasks to adjust treatment plans dynamically in response to changes in patient anatomy and tumor characteristics during the course of treatment (9, 23). AI-driven methods, particularly deep learning and generative approaches, facilitate this by enabling synthetic CT generation from cone-beam CTs or CBCT-based co-registration with planning CTs, as the basis for re-planning in short timeframes and at high quality (21, 23). Furthermore, autosegmentation of OARs and target volumes provides rapid and more reproducible contouring, thereby reducing the practical barrier to online or offline adaptation (5, 9).
More recently, AI has also been used to support the selection of adaptive strategies and to identify patients who are most likely to benefit from ART. Models trained on radiomic, volumetric, or clinical features may predict the need for adaptation due to anatomical changes, thereby supporting more efficient resource allocation (23–25). In this context, AI should not be seen only as a tool for accelerating individual tasks, but increasingly as an enabler of clinically feasible adaptive workflows across the full chain from imaging to contouring, dose recalculation, plan selection, and quality control.
Motion management
Motion management remains a cornerstone for precision in radiation therapy, especially for tumors in the thorax and abdomen, where respiration and internal organ deformation can degrade dose delivery. Recent studies illustrate how AI is being leveraged across several sub-domains: tumor tracking, respiratory gating and motion prediction, and deformable image registration (26–28).
For tumor tracking, deep learning has been applied to cine MRI and fluoroscopic sequences to achieve real-time localization (26, 27). In respiratory gating, AI-driven motion prediction has been explored to reduce system latency, with temporal models showing promise for forecasting tumor motion trajectories (26, 28). In the context of any motion-management approach, deformable image registration and deformation compensation remain key. Here, AI-based solutions have shown improved speed and, in selected settings, improved performance over conventional methods (28).
At the same time, this field remains highly translational. Robustness to imaging quality, generalizability across treatment systems, and clinically meaningful evaluation under realistic motion conditions remain important challenges. Nonetheless, motion management is one of the clearest examples of how AI may contribute not only to workflow efficiency, but directly to treatment precision upon irradiation (26–28).
MR-only workflows
The availability of MR-guided radiotherapy has enabled adaptive radiotherapy across several tumor sites where superior soft-tissue contrast improves target and OAR localization. Building on this foundation, there is growing interest in MR-only workflows that streamline treatment by eliminating the need for CT, reducing registration errors, and shortening patient visits, ultimately improving workflow efficiency and patient experience (21, 22, 29).
A central challenge is the absence of electron density information in MRI, which is critical for dose calculation. Here, synthetic CTs from MRI data have emerged as a key enabler. Fueled by an active community and dedicated AI challenges (30), deep learning models trained to map MR intensities to pseudo-CT images have demonstrated clinically relevant dosimetric accuracy in several disease sites (21, 22, 29). Prospective and implementation-oriented studies increasingly support the feasibility of MR-only planning in selected indications (22, 31).
Beyond synthetic CT generation, AI can further enhance MR-only workflows through auto-segmentation of targets and OARs directly on MR images, image-quality monitoring, and automated quality assurance to detect artifacts or geometric distortions (21, 31). Together, these tools pave the way for efficient MR-only adaptive workflows, in which AI is essential not only for speed, but also for robustness and clinical adoption.
Biology-adapted radiotherapy
While AI-enabled automation from segmentation to automated planning and adaptive radiotherapy concepts have already arrived in clinical practice, clinical concepts enabling biology-adapted radiotherapy remain limited despite strong potential for optimization in terms of personalized fractionation, spatial dose shaping, and target and OAR dose prescriptions or constraints (24, 32, 33). The growing molecular characterization of tumors and increasing understanding of phenotypic tumor representation driven by the tumor microenvironment allow for quantification of these objectives. Computational methods, and in particular AI solutions capable of accounting for the variety of input data types encompassing imaging, histopathology, clinical history, and multi-omics characterization, are key enablers of biology-adapted radiotherapy and future clinical decision-support systems (33, 34).
This paradigm promises more precise prediction of tumor response and adaptive strategies to improve outcomes while minimizing toxicity. However, multimodal prediction in radiotherapy remains challenging. Two factors currently limit the translation of the success of AI for automation in RT to biology-adapted RT: the quality and completeness of input data, and the reliability of outcome labels (33, 34). For this reason, the biology-adapted side of AI in radiation oncology currently remains scientifically very active, but clinically less mature than workflow automation.
Multimodal learning and data integration
Real-world clinical datasets are sparse, limited in sample size, and heterogeneous across institutions, reflecting variability in imaging protocols, sequencing platforms, pathology workflows, and electronic health-record documentation (32, 34). Importantly, data are often not missing at random: advanced imaging or molecular profiling is typically ordered selectively, introducing systematic biases. While early AI solutions were often developed on curated complete-case datasets, more modern architectures increasingly incorporate mechanisms to handle missingness, asynchronous modalities, and irregular sampling (35, 36).
Approaches such as multimodal fusion networks, cross-modal transformers, and foundation-style models have shown promise because they allow flexible aggregation of variable input streams and align more closely with the realities of radiation-oncology data (34, 36). In parallel, the increasing availability of pretrained data-domain specific (foundation) models across imaging, pathology, and text may help to address data limitations by providing transferable feature representations that can be fine-tuned for specific radiotherapy tasks such as response prediction or toxicity modeling (35, 37). However, model interpretability and trustworthiness remain major concerns given a more challenging process for regulatory approval in the absence of human oversight (as is the case for task automation). Hybrid approaches that combine data-driven AI with mechanistic or radiobiological priors may therefore offer a particularly attractive translational path (33, 37).
The importance of well-defined prediction objectives
In addition to input features, outcome labels such as tumor control, spatiotemporal response patterns, recurrence, or normal tissue toxicity are equally important for the successful implementation of biology-adapted radiotherapy. However, these endpoints remain difficult to quantify reliably and reproducibly (33,38). Both input-data breadth and label reliability jointly complicate the development and validation of robust AI-driven prognostic models and limit their generalizability. It will therefore be important to tailor AI solutions specifically to these data realities, implying a need for dedicated AI-in-RT outcome-prediction strategies rather than direct transfer of methods optimized for automation tasks (33, 34, 38).
Despite these challenges, several successful applications have recently emerged. Particularly interesting are dose-painting concepts informed by recurrence prediction and multimodal prognosis models that combine imaging with clinical variables (38–41). More recent studies in head-and-neck cancer illustrate that multimodal fusion may improve prognostic prediction and radiotherapy-response assessment compared with unimodal approaches (38, 39). These models do not yet translate directly into validated dose-painting protocols, but they do illustrate how AI-derived risk maps could ultimately guide selective spatial dose escalation and motivate prospective clinical trials.
Biology-informed CTV definitions
While automation has already been adopted for OAR delineation and, to some extent, gross tumor volume delineation, automated accounting for microscopic tumor spread on imaging, that is, CTV definition, remains challenging despite increasing evidence from both mechanistic and AI-driven work (40, 42). While selected applications aim for purely data driven solutions building on large-scale data to abstract complex infiltration patterns (43–45), mechanistic approaches rooted in reaction-diffusion or proliferation-invasion physics actively simulate tumor-cell migration and may generate anisotropic risk maps that better reflect microscopic spread than uniform geometric margins (41, 46). Complementing this, AI methods, including radiomics and deep learning, can extract peritumoral phenotypes from routine imaging to estimate occult disease extension (47–49). Similar concepts are hence emerging in glioma and head-and-neck cancer, where machine-learning models may help personalize target definition and account for likely microscopic spread along biologically plausible pathways.
Taken together, mechanistic simulations and AI predictors provide converging evidence that target volumes may eventually be biologically individualized. Translation will require prospective validation, standardized imaging, and integration into treatment planning systems, but the methodological groundwork is increasingly substantial.
Interactive and agent-based AI
The rapid adoption of large language models has given rise to strong interest in agent-based AI systems, interactive tools designed to assist users rather than replace human decision-making. In radiation oncology, these systems may streamline routine tasks such as report or letter writing, patient summarization, information extraction from unstructured records, and trial or treatment-option exploration based on clinician-entered features, potentially with multimodal inputs (50–52). Unlike more traditional AI focused on automation or prediction, agent-based models are inherently human-in-the-loop, allowing users to query, refine, or challenge outputs.
There is growing literature supporting such applications. Recent work has shown that locally deployed LLMs can generate physician letters in institution-specific style and summarize radiation-oncology workflow documents with high clinician acceptability (53, 54). These studies are particularly relevant because they move the discussion from generic chatbot performance toward concrete, radiation-oncology-specific workflow tasks. More broadly, current radiology and oncology literature suggests that retrieval-augmented generation, local deployment, and task-constrained use are likely to be more relevant for near-term clinical translation than unconstrained chatbot use (55–57).
Despite this promise, several key hurdles still limit clinical translation. Data privacy and security remain paramount, particularly because many models are cloud-based and depend on transfer of sensitive data. Local deployment or on-premise hosting can mitigate this but requires infrastructure and governance (58–60). There is also the issue of trust: outputs must be accurate, current, explainable, and appropriately sourced, and hallucinations remain a central concern. From a workflow perspective, integration into EHRs and treatment-planning systems, interface design, user training, and regulatory oversight are all necessary. In the near term, the most realistic role of agent-based AI in radiation oncology is therefore supervised documentation support, information synthesis, and constrained decision support rather than autonomous clinical action (13, 61, 62).
QA and QC of AI
With the growing application of AI solutions in clinical practice, efforts to assess and ensure their quality are as critical as model development itself. Traditional quality assurance in radiation oncology focuses on validating outputs prior to clinical use, for example, human verification of auto-segmentation or adherence of automated plans to established QA protocols before treatment delivery. While these remain necessary, AI-specific QA must extend to decision support and human-AI interaction, particularly in mitigating automation bias. If clinicians defer too strongly to AI outputs without scrutiny, safety risks can emerge even when underlying algorithms perform well in benchmark settings (63, 64).
In auto-segmentation, QA frameworks have been proposed that combine geometric accuracy, clinical acceptability, time efficiency, and dosimetric relevance, moving beyond single-metric evaluation (7, 14). Parallel efforts address prediction confidence: calibration methods aim to align model certainty with output correctness, ensuring that incorrect predictions are accompanied by lower confidence and therefore prompt human review (15, 65). Another major emerging dimension is uncertainty quantification. Bayesian deep learning, ensemble modeling, test-time augmentation, and out-of-distribution detection are examples of methods used to capture uncertainty arising from limited training data, anatomical variation, or unexpected inputs (15, 65). Proper handling of such uncertainty is essential for clinical deployment, since it allows AI systems not only to predict, but also to indicate when they may fail.
More recent work has also moved toward practical implementation of automated contour QA in multicenter settings and toward broader frameworks for trustworthy AI in radiotherapy (66). These developments indicate that QA and QC are no longer only downstream verification steps, but increasingly integral parts of AI-system design, implementation, and long-term monitoring.
Outlook and conclusions
Radiation oncology has historically been at the forefront of technological innovation, integrating imaging, physics, and clinical sciences to advance cancer care. AI now represents the next major transformative force, with demonstrated utility in automation of segmentation, planning, dose prediction, and adaptive workflows. These domains highlight how AI can improve efficiency, consistency, and safety while freeing clinical experts to focus on individualized decision-making. More recent efforts extend beyond automation toward biology-informed adaptation, multimodal prediction, and interactive agent-based solutions, underscoring the role of AI in enabling more personalized and comprehensive cancer care.
Despite this progress, several hurdles must be addressed before AI can be fully embedded into routine clinical practice. Access to high-quality, large-scale, and harmonized datasets remains a major bottleneck, particularly for multimodal and longitudinal applications. External validation, prospective evidence, generalizability across institutions, and trustworthy integration into clinical workflows remain insufficient for many proposed tools. Equally important is building trust through robust quality assurance, uncertainty quantification, continuous monitoring, and clear human oversight. Regulatory frameworks must adapt to AI’s iterative nature, and implementation science will become increasingly important as tools move from single-center development to routine deployment.
Finally, the long-term vision of AI in radiation oncology should align with comprehensive cancer care: integrating multimodal clinical, imaging, pathological, and molecular data to guide not only radiotherapy, but also systemic therapy integration, survivorship, and long-term follow-up. In this context, AI should be regarded not as a replacement for clinical expertise but as a catalyst for multidisciplinary, biology-driven, and patient-centered cancer care.
Use of artificial intelligence: Artificial intelligence tools were used to assist with language editing, stylistic revision, restructuring of text, and development of figure concepts. All content was reviewed, revised, and approved by the authors, who take full responsibility for the final manuscript.
Use of artificial intelligence
Artificial intelligence tools were used to assist with language editing, stylistic revision, restructuring of text, and development of figure concepts. All content was reviewed, revised, and approved by the authors, who take full responsibility for the final manuscript.
Copyright
Aerzteverlag medinfo AG
– Department of Radiation Oncology, Inselspital, Bern University Hospital, and University of Bern, Switzerland
– Department of Digital Medicine, University of Bern, Switzerland
Department of Radiotherapy, University of Groningen, University Medical Center Groningen, Groningen, the Netherlands.
Department of Digital Medicine, University of Bern, Switzerland
The authors have not disclosed any conflicts of interest related to this article.
1. Topol, E. J. High-performance medicine: the convergence of human and artificial intelligence. Nat. Med. 25, 44–56 (2019).
2. Hosny, A., Parmar, C., Quackenbush, J., Schwartz, L. H. & Aerts, H. Artificial intelligence in radiology. Nat Rev Cancer 18, 500–510 (2018).
3. Conroy, L. et al. Artificial intelligence for radiation treatment planning: Bridging gaps from retrospective promise to clinical reality. Clin. Oncol. (R Coll. Radiol.) 37, 103630 (2025).
4. Jeong, C., Goh, Y. & Kwak, J. Challenges and opportunities to integrate artificial intelligence in radiation oncology: a narrative review. Ewha Med. J. 47, e49 (2024).
5. Erdur, A. C. et al. Deep learning for autosegmentation for radiotherapy treatment planning: State-of-the-art and novel perspectives. Strahlenther. Onkol. 201, 236–254 (2025).
6. Poel, R. et al. A comprehensive multifaceted technical evaluation framework for implementation of auto-segmentation models in radiotherapy. Commun. Med. (Lond.) 5, 319 (2025).
7. Wahid, K. A. Artificial intelligence uncertainty quantification in radiotherapy applications: a scoping review. Radiother Oncol (2024).
8. Ronneberger, O., Fischer, P. & Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. arXiv [cs.CV] (2015) doi:10.48550/arXiv.1505.04597.
9. Mastella, E. A systematic review of the role of artificial intelligence in CT-based adaptive radiotherapy for head and neck cancer. Phys Imaging Radiat Oncol (2025).
10. Isensee, F., Jaeger, P. F., Kohl, S. A. A., Petersen, J. & Maier-Hein, K. H. nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation. Nat. Methods 18, 203–211 (2021).
11. Mackay, K., Bernstein, D., Glocker, B., Kamnitsas, K. & Taylor, A. A review of the metrics used to assess auto-contouring systems in radiotherapy. Clin. Oncol. (R Coll. Radiol.) 35, 354–369 (2023).
12. Albertini, F., McWilliam, A. & Winey, B. Editorial: Advances in online and real-time adaptive radiotherapy. Phys. Med. Biol. 70, 070301 (2025).
13. Guo, Y. et al. Deep learning for CT synthesis in radiotherapy. Bioengineering (Basel) 12, 1297 (2025).
14. Zhu, L. et al. Establishing prospective performance monitoring for real-world implementation of deep learning-based auto-segmentation in prostate cancer radiotherapy. Phys. Imaging Radiat. Oncol. 36, 100886 (2025).
15. Hémon, C., Texier, B., Lafond, C., Nunes, J.-C. & Barateau, A. Towards trustworthy AI in radiotherapy: a comprehensive review of uncertainty-aware techniques. Phys. Med. Biol. 71, 01TR01 (2025).
16. Ge, Y. & Wu, Q. J. Knowledge-based planning for intensity-modulated radiation therapy: a literature review. J Appl Clin Med Phys 20, 12–29 (2019).
17. Yu, L. et al. Multicenter study on the versatility and adoption of AI-driven automated radiotherapy planning across cancer types. Nat. Commun. 17, 867 (2025).
18. Kazemzadeh, A., Rasti, R. & Tavakoli, M. B. Artificial intelligence for radiotherapy dose prediction: A comprehensive review. Cancer Radiother. 29, 104630 (2025).
19. Momin, S. et al. Knowledge-based radiation treatment planning: A data-driven method survey. J. Appl. Clin. Med. Phys. 22, 16–44 (2021).
20. Chung, C. V. et al. Knowledge-based planning for fully automated radiation therapy treatment planning of 10 different cancer sites. Radiother. Oncol. 202, 110609 (2025).
21. Spadea, M. F., Maspero, M., Zaffino, P. & Seco, J. Deep learning based synthetic-CT generation in radiotherapy and PET: A review. Med. Phys. 48, 6537–6566 (2021).
22. Deng, J. et al. Development and clinical implementation of an MRI-only planning workflow featuring deep learning-based synthetic CT for prostate cancer external beam radiotherapy. J. Appl. Clin. Med. Phys. 26, e70228 (2025).
23. McCullum, L. et al. Review: Adaptive radiation therapy for head and neck cancer. arXiv [physics.med-ph] (2025) doi:10.48550/arXiv.2508.00651.
24. Lambin, P. et al. Radiomics: the bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 14, 749–762 (2017).
25. Tian, R. et al. Multimodal fusion model for prognostic prediction and radiotherapy response assessment in head and neck squamous cell carcinoma. NPJ Digit. Med. 8, 302 (2025).
26. Lombardo, M. Patient-specific deep learning tumor tracking for cine MRI in MR-guided radiotherapy. Radiother Oncol (2025).
27. Wang, Y. A clinical dataset for real-time tumor tracking for MRI-guided radiotherapy. Sci Data (2025).
28. Fu, Y. et al. Deep learning in medical image registration: a review. Phys. Med. Biol. 65, 20TR01 (2020).
29. Pereira, D. Applicability of MRI-only technique in external beam radiotherapy: dosimetric evaluation, IGRT, and quality assurance-a systematic review. Phys Imaging Radiat Oncol (2025).
30. Xiao, F. et al. DoseRAD2026 Challenge dataset: AI accelerated photon and proton dose calculation for radiotherapy. arXiv [physics.med-ph] (2026) doi:10.48550/arXiv.2604.12778.
31. Earwong, P. Clinical implementation of deep learning-based synthetic CT in MRI-only radiotherapy workflows. Radiol Artif Intell (2025).
32. Huang, S. C. Multimodal foundation models in medicine: a systematic review and implementation guidance. NPJ Digit Med (2025).
33. Deist, T. M., Dankers, F. & Ojha, P. Machine learning algorithms for outcome prediction in head and neck cancer: a systematic review. Lancet Oncol 19, e419–e431 (2018).
34. Sanduleanu, S. et al. Tracking tumor biology with radiomics: A systematic review utilizing a radiomics quality score. Radiother. Oncol. 127, 349–360 (2018).
35. Paschali, M. et al. Foundation models in radiology: What, how, why, and why not. Radiology 314, e240597 (2025).
36. Tavakoli, N. et al. Generative AI and foundation models in radiology: Applications, opportunities, and potential challenges. Radiology 317, e242961 (2025).
37. Bian, Y., Li, J., Ye, C., Jia, X. & Yang, Q. Artificial intelligence in medical imaging: From task-specific models to large-scale foundation models. Chin. Med. J. (Engl.) 138, 651–663 (2025).
38. Deist, T. M. & Dekker, A. Outcome modelling and response prediction in radiation oncology. Clin Transl Radiat Oncol (2025).
39. Parmar, C., Leijenaar, R. & Grossmann, P. Radiomic feature clusters and prognostic signatures specific for lung and head-and-neck cancer. Sci Rep 5, (2015).
40. Rockne, R. Reaction-diffusion and proliferation-invasion modeling of glioma spread. Math Biosci Eng (2010).
41. Swanson, K. R. Quantitative modeling of glioma growth and invasion. J Neurol Sci (2008).
42. Tran, N. et al. Novel radiotherapy target definition using AI-driven predictions of glioblastoma recurrence from metabolic and diffusion MRI. NPJ Digit. Med. 8, 508 (2025).
43. Matoska, T., Patel, M., Liu, H. & Beriwal, S. Review of deep learning based autosegmentation for clinical target volume: Current status and future directions. Adv. Radiat. Oncol. 9, 101470 (2024).
44. Ma, C.-Y. et al. Deep learning-based auto-segmentation of clinical target volumes for radiotherapy treatment of cervical cancer. J. Appl. Clin. Med. Phys. 23, e13470 (2022).
45. Huang, S. et al. Auto-segmentation and auto-planning in automated radiotherapy for prostate cancer. Bioengineering (Basel) 12, 620 (2025).
46. Lipková, J., Menze, B., Wiestler, B., Koumoutsakos, P. & Lowengrub, J. S. Modelling glioma progression, mass effect and intracranial pressure in patient anatomy. J. R. Soc. Interface 19, 20210922 (2022).
47. Cepeda, S. et al. Radiomics-based quantification of tumor infiltration in the non-enhancing peritumoral region on postoperative MRI is associated with survival in glioblastoma. Sci. Rep. 15, 43932 (2025).
48. Chen, X. et al. Habitat radiomics predicts occult lymph node metastasis and uncovers immune microenvironment of head and neck cancer. J. Transl. Med. 23, 498 (2025).
49. Lan, T. et al. MRI-based deep learning and radiomics for prediction of occult cervical lymph node metastasis and prognosis in early-stage oral and oropharyngeal squamous cell carcinoma: a diagnostic study. Int. J. Surg. 110, 4648–4659 (2024).
50. Hou, Y. Fine-Tuning a Local LLaMA-3 Large Language Model for Radiation Oncology Physician Letters. Front Artif Intell. (2025).
51. Cao, M. et al. Evaluating the performance of using large language models to automate summarization of CT simulation orders in radiation oncology. Int. J. Radiat. Oncol. Biol. Phys. 123, e13–e14 (2025).
52. Dennstädt, F. Comparative evaluation of a medical large language model on real-life questions from radiation oncology practice. Strahlenther Onkol (2025).
53. Cao, M. et al. Using large language models to automate summarization of CT simulation orders in radiation oncology. J. Appl. Clin. Med. Phys. 26, e70310 (2025).
54. Holmes, J. et al. RadOnc-GPT: An autonomous LLM agent for real-time patient outcomes labeling at scale. arXiv [cs.AI] (2025) doi:10.48550/arXiv.2509.25540.
55. Patwardhan, V. Leveraging large language models to enhance radiology and oncology workflow: practical guidance and research priorities. J Am Coll Radiol (2025).
56. Kadoya, N. et al. Evaluating the capability of large language models in radiotherapy through professional certification examinations in Japan. J. Radiat. Res. 67, 114–120 (2026).
57. Bluethgen, C. et al. Best practices for large language models in radiology. Radiology 315, e240528 (2025).
58. Rajendran, P. et al. Large language model-augmented learning for auto-delineation of treatment targets in head-and-neck cancer radiotherapy. Radiother. Oncol. 205, 110740 (2025).
59. Yalamanchili, A. et al. Quality of large language model responses to radiation oncology patient care questions. JAMA Netw. Open 7, e244630 (2024).
60. Fu, J., Cheng, Y., Li, Z. & Fu, J. Intelligent support for radiotherapy: A review of clinical applications for large language models. J. Clin. Med. 15, 2531 (2026).
61. Recent Trends of Artificial Intelligence in Radiation Oncology: A Narrative Review of Prospective Studies.
62. Zhao, L. et al. AI agent in healthcare: applications, evaluations, and future directions. NPJ Artif. Intell. 2, (2026).
63. Jafar, A. & Jia, X. Towards human-centric intelligent treatment planning for radiation therapy. NPJ Digit. Med. 9, 155 (2026).
64. Heising, L. M. et al. Maximizing impact of explainable artificial intelligence in radiotherapy: a critical review. Phys. Med. Biol. 71, (2026).
65. Van Aalst, J. E. Reliability of uncertainty quantification methods for deep-learning radiotherapy applications. Med Phys (2025).
66. Chlap, P. Implementation of an automated contour quality assurance tool within a multicenter radiotherapy trial. Radiother Oncol (2025).



info@onco-suisse
- Vol. 16
- Ausgabe 3
- Juni 2026