En dépit des maux qui, avec l’ âge, affectent le corps, vieillir demeure un privilège dont sont privés celles et ceux que fauchent prématurément la maladie, la famine ou la guerre. Mais plus un individu vieillit, plus s’ accroît la probabilité pour lui d’ être atteint de maladies dont chacune va imposer le recours à un ou plusieurs médicaments. Ainsi par exemple, le traitement actuel de l’ insuffisance cardiaque propose à lui seul quatre substances fondamentales. Appliquée sans discernement à des individus polymorbides, l’ Evidence Based Medicine ne peut qu’ aggraver la situation.
Or, paradoxe naturel, un organisme âgé demande davantage de médicaments alors qu’ il est plus vulnérable à leurs effets secondaires et à leurs interactions qui, non identifiés, risquent d’ accroître la polymédication par une prescription supplémentaire indue censée les traiter.
La consultation du Compendium suisse démontre qu’ en la matière, « tous peuvent tout faire ». A l’ inverse, comme l’ exprimait Georges Peters (1920-2006) ancien professeur de pharmacologie à la Faculté de médecine de Lausanne : « Si un médicament n’ a pas d’ effet secondaire, c’ est qu’ il n’ a pas d’ effet primaire ».
Après que l’ attention fut portée, notamment dans des établissements médico-sociaux, sur la polypharmacie atteignant parfois jusqu’ à 13 produits différents par personne et par jour (1,2) apparut la nécessité d’ une « déprescription », néologisme signifiant la suppression des médicaments jugés inappropriés ou inutiles (3,4). Bien qu’ indispensable, cette démarche reste insuffisante car il convient encore d’ identifier le médicament à l’ origine d’ un effet indésirable ou sans action thérapeutique. C’ est tout l’ intérêt du test de phénotypage, mesure in vivo de l’ activité enzymatique des cytochromes P450 et d’ un transporteur comme la glycoprotéine P (P-gp). Les premiers transforment les médicaments pour en faciliter l’ élimination et la seconde limite l’ absorption de nombreuses substances qu’ elle contribue à évacuer. Le test consiste à administrer oralement un médicament métabolisé par l’ enzyme dont on veut savoir l’ activité. Le résultat, donné par l’ analyse des métabolites, identifie un phénotype normal (activité enzymatique attendue), intermédiaire (activité enzymatique diminuée), lent (activité enzymatique très réduite ou absente) ou ultrarapide (activité enzymatique augmentée) (5).
En regard d’ une résistance thérapeutique ou au contraire d’ une hypersensibilité aux médicaments, « le phénotype mesuré par l’ examen et la réponse clinique du patient permet ainsi d’ adapter le traitement en modifiant les posologies ou en changeant de molécules » (5).
Les tests pharmacogénomiques, encore trop peu demandés en gériatrie malgré leur intérêt pour la population âgée, s’ avèrent désormais un des piliers du primum non nocere.
1. Silva C, Ramalho C, Luz I, Monteiro J et al. Drug-related problems
in institutionalized, polymedicated elderly patients: opportunities for
pharmacist intervention. Int J Clin Pharm 2015;37:327-34.
2. Fog AF, Kvalvaag G, Engedal K, Strand J. Drug-related problems and changes in drug utilization after medication reviews in nursing homes
in Oslo, Norway. Scand J Prim Health Care 2017; 35:329-35.
3. Cateau D, Foley RA, Niquille A. Déprescrire en EMS: regards croisés entre les résidents, leurs proches et les professionnels de la santé.
Rev Med Suisse 2020;16:2169-71.
4. Blum MR, Sallevelt BTGM, Spinewine A, O’Mahony D et al. Optimizing
Therapy to Prevent Avoidable Hospital Admissions in Multimorbid
Older Adults (OPERAM): cluster randomised controlled trial. BMJ 2021;374:n1585.
5. El Biali M, Rollason V, Desmeules J, Samer C. Phénotypage en gériatrie : le « Geneva cocktail » comme aide à la prescription médicamenteuse. La gazette médicale 2022;11:14-16.
Le surpoids et l’ obésité représentent l’ un des plus grands défis mondiaux pour le système de santé de notre époque (1-4). Selon les derniers chiffres du « Rapport régional européen de l’ OMS sur l’ obésité 2022 », près de 60 % des adultes et 1/3 des enfants en Europe sont déjà touchés par le surpoids ou l’ obésité (5) – et les chiffres en Europe et dans le monde continuent d’ augmenter. L’ obésité est un facteur de risque majeur pour de nombreuses maladies telles que les maladies cardio-vasculaires, le diabète de type 2 et les cancers les plus divers, et elle est associée à une mortalité accrue (6, 7). Pour enrayer l’ épidémie d’ obésité actuelle et future, il est important de comprendre que l’ obésité est une maladie et que les personnes souffrant d’ obésité ont besoin d’ un traitement spécifique et sur mesure.
Obesity represents a global socioeconomic health burden with epidemic dimensions worldwide (1-4). According to the WHO European Regional Obesity Reports 2022, already now 60% or adults and 1/3 of all children are affected in Europe (5) – and the numbers keep increasing in Europe and worldwide. Obesity is a major risk factor for multiple comorbidities such as type 2 diabetes, cardiovascular disease and cancer, and is associated with an increased overall mortality (6, 7). To successfully fight this epidemic now and in the future, it is important to understand that obesity is a disease and that people with obesity need a specific, tailored treatment. Key Words: obesity, GLP-1 analogues, stigmatization, tailored treatment
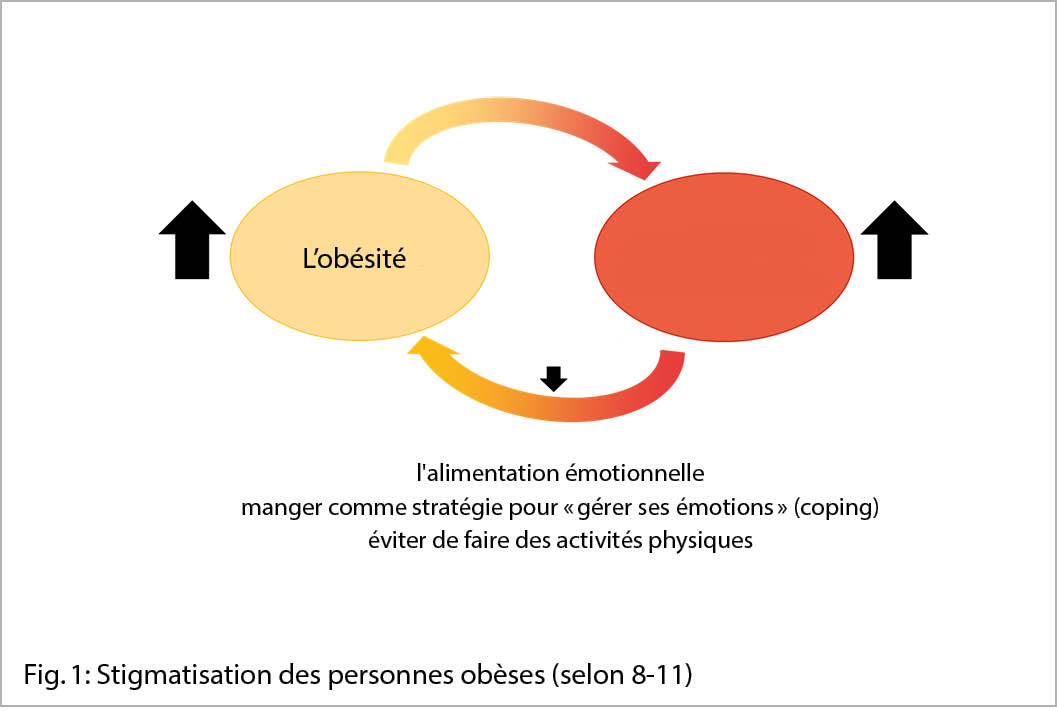
Il est dramatique de constater que l’ idée fausse selon laquelle le surpoids et l’ obésité résultent d’ un manque d’ effort et de volonté et que les personnes concernées doivent « simplement faire plus d’ efforts, manger moins et bouger plus » est encore largement répandue. Cela a pour conséquence que les personnes souffrant d’ obésité subissent une stigmatisation massive, non seulement dans notre société, mais aussi et surtout dans le secteur de la santé. Cette stigmatisation se fait d’ abord ressentir à l’ extérieur et s’ intériorise avec le temps, c’ est-à-dire que les personnes obèses se font très souvent de gros reproches sur l’ évolution de leur poids et se dévalorisent elles-mêmes. Cela entraîne un cercle dangereux qui est à la fois la conséquence et la cause de l’ obésité et qui favorise les comportements alimentaires émotionnels. La nourriture représente un moyen de « gérer ses émotions » (coping) et les personnes concernées évitent de se montrer dehors pour faire du sport car cela engendre encore plus de stress psychologique (fig. 1).
La stigmatisation dans le secteur de la santé et par les médecins, qui a été vécue au moins une fois par près de 70 % des personnes concernées dans une grande étude multinationale et multicentrique (12), peut avoir des conséquences graves telles qu’ un éloignement complet du système de santé, un abus de substances et une suicidalité accrue (12-14).
Diagnostic et pathogenèse
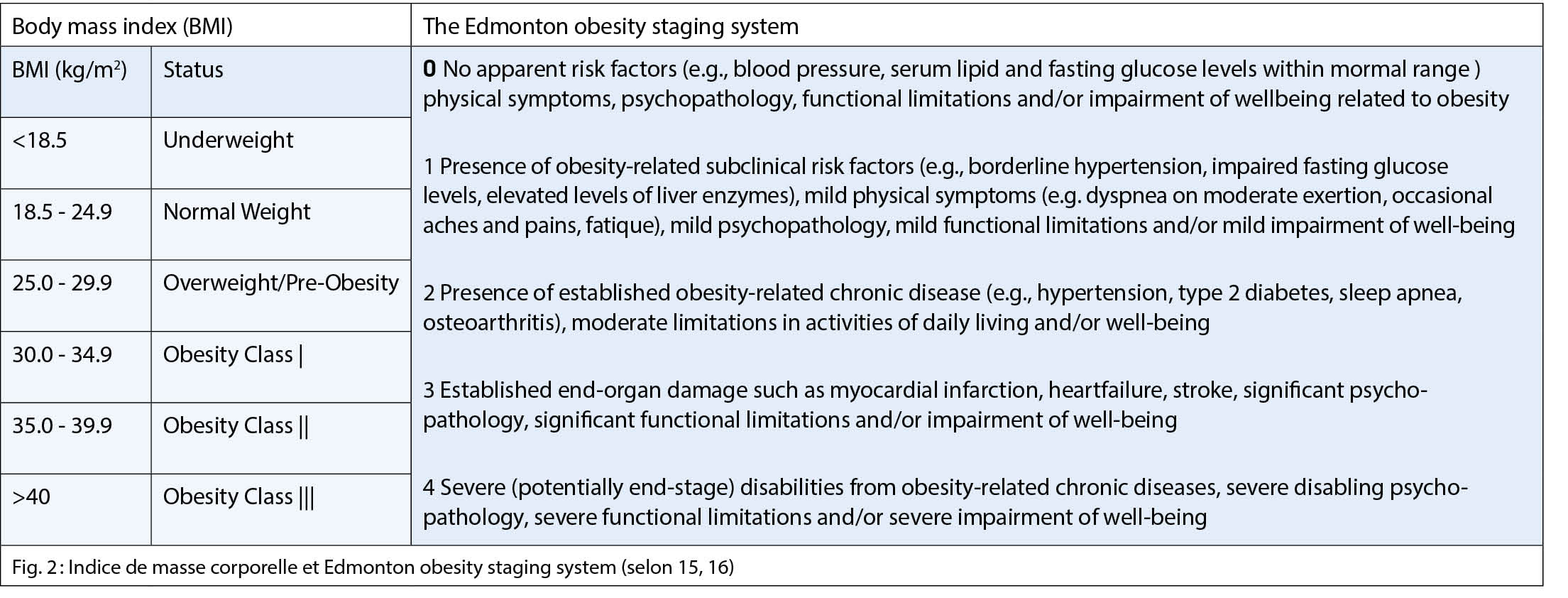
Le surpoids et l’ obésité sont largement classifiés selon l’ indice de masse corporelle (IMC, kg/m2), bien qu’ il ne s’ agisse que d’ une classification très vague, qui peut être complétée par l’ application supplémentaire du « Endmonton obesity staging system », qui tient compte des maladies suite à l’ obésité (fig. 2).
L’ obésité est une maladie multifactorielle, c’ est-à-dire que des facteurs (épi)génétiques, (neuro)biologiques et externes, appelés facteurs de « style de vie », jouent un rôle. Les processus neurobiologiques modifiés jouent ici un rôle décisif, car le cerveau détermine de manière largement autonome ce que nous mangeons, quand et comment nous le faisons, et comment se déroulent nos processus métaboliques. Ces processus, comme beaucoup d’ autres processus du corps humain, ne peuvent être influencés que de manière très marginale par la volonté. En d’ autres termes, le patient souffrant d’ obésité n’ est pas en surpoids parce qu’ il mange trop, il mange trop parce qu’ il est atteint d’ obésité !
Traitement de l’ obésité avec des analogues du GLP-1
Aujourd’ hui encore, une alimentation adaptée et équilibrée et suffisamment d’ activité physique sont les piliers du traitement de l’ obésité. Mais l’ obésité doit avant tout être traitée là où elle se développe, c’ est-à-dire au niveau neurobiologique. Avec les analogues du GLP-1, nous disposons pour la première fois dans l’ histoire du traitement de l’ obésité de médicaments qui nous permettent de traiter l’ obésité de manière ciblée, avec une bonne tolérance et des effets secondaires acceptables. Les analogues du GLP-1 provoquent au niveau du cerveau un renforcement de la sensation de satiété et une diminution de la sensation de faim, ce qui fait que l’ on mange moins. Des études ont montré une diminution moyenne du poids corporel de 10 % par rapport au poids initial (17,18). Les effets individuels peuvent toutefois être plus ou moins importants.
Les patients sous traitement avec des analogues du GLP-1 mentionnent surtout qu’ ils sont plus vite rassasiés et qu’ ils ne veulent ou ne peuvent plus manger que de petites portions. De nombreux patients affirment ressentir une grande détente générale, car ils ne doivent plus dépenser autant d’ énergie pour « éviter de manger ». Outre la réduction du poids, le traitement par les analogues du GLP-1 a d’ autres effets positifs sur les processus métaboliques, par exemple au niveau du foie, et a aussi des effets positifs sur le système cardiovasculaire.
En Suisse, l’ analogue du GLP-1, le liraglutide (Saxenda®), est autorisé pour le traitement de l’ obésité. Les coûts d’ un traitement avec l’ analogue du GLP-1 liraglutide (Saxenda®) sont pris en charge par la caisse maladie en Suisse depuis le 01.04.2020 sous certaines conditions. Il est important de savoir que ce médicament ne peut être prescrit que par des médecins endocrinologues/diabétologues FMH ou des spécialistes de l’ obésité (selon la liste de l’ OFSP). Cela signifie que les patients doivent être envoyés aux spécialistes concernés pour un traitement.
Les conditions pour une prise en charge des coûts du traitement avec l’ analogue du GLP-1 Saxenda® (liraglutide) sont les suivantes :
IMC ≥ 28kg/m2 avec pathologies associées liées au poids (prédiabète, diabète sucré de type 2, dyslipidémie, hypertension artérielle) OU
IMC ≥ 35kg/m2 indépendamment de pathologies associées.
Suivi approuvé d’ un régime déficitaire de 500kcal par jour.
Augmentation documentée de l’ activité physique, par ex. à l’ aide d’ un compteur de pas.
Contrôle des résultats et décision concernant la poursuite de la prise en charge des coûts au bout de 4 mois et ensuite tous les 6 mois
Prise en charge des coûts pendant 3 ans maximum
Le liraglutide (Saxenda®) doit être injecté quotidiennement par le patient par voie sous-cutanée. L’ injection est simple et se fait à l’ aide d’ un stylo. Il est toutefois important de bien instruire le patient concernant la technique d’ injection correcte. Il est également important de commencer par une faible dose (0,6mg/jour) et de n’ augmenter la dose que lentement, chaque semaine, jusqu’ à une dose maximale de 3mg par jour, afin de permettre au corps de s’ habituer lentement au médicament. Ainsi, les effets secondaires possibles tels que les nausées et, très rarement, les vomissements peuvent être minimisés ou totalement évités. D’ autres effets secondaires possibles sont la diarrhée ou la constipation. Tout comme la réponse au médicament, l’ émergence d’ effets secondaires varie considérablement d’ un patient à l’ autre.
Outre le traitement par des analogues du GLP-1, la chirurgie bariatrique représente pour des patients sélectionnés une méthode très efficace et sûre de réduction de poids. Ainsi on peut traiter ou même guérir complètement les maladies associées à l’ obésité. Quelle que soit la forme de thérapie, le patient doit être au centre du traitement et il faut trouver une approche individuelle et sur mesure pour chaque patient. Pour qu’ un traitement de l’ obésité soit efficace, il faut plutôt suivre la devise « state of the heart » que « state of the art » : le patient doit sentir que l’ on prend en compte ses besoins et ses souhaits individuels et qu’ il est perçu dans la réalité de la vie avec son vécu.
Cet article est une traduction de « der informierte arzt » 09_2022
Copyright Aerzteverlag medinfo AG
Pre Katharina Timper
Clinique d’endocrinologie, de diabétologie et
de métabolisme Hôpital universitaire de Bâle
Petersgraben 4
4031 Bâle
Département de biomédecine, Université de Bâle
L’ auteur n’ a pas déclaré de conflits d’ intérêts en rapport avec cet article.
◆ L’ obésité est une maladie ➞ Les patients souffrant d’ obésité ont besoin d’ un traitement spécifique.
◆ « State of the heart » : une attitude respectueuse, empathique et non stigmatisante envers le patient est primordiale, Entretien motivationnel – médecin-patient=équipe.
◆ Prise en compte : des troubles alimentaires, de l’ alimentation émotionnelle, de la santé mentale, du classement de l’ obésité (IMC et Edmonton Obesity Scale), des maladies associées à l’ obésité ; exclusion de causes endocrinologiques de l’ obésité.
◆ Établir ensemble avec le patient un plan d’ action et de traitement incluant les objectifs de celui-ci.
◆ Élaborer des changements de mode de vie pour chaque patient et les mettre en pratique de manière interdisciplinaire (avec éventuellement le transfert du patient à un centre de l’ obésité).
◆ Traiter l’ obésité de manière ciblée avec des analogues du GLP-1
(consultation d’ un médecin endocrinologue/diabétologue FMH ou d’ un spécialiste de l’ obésité selon la liste de l’ OFSP).
◆ Prendre en considération la chirurgie bariatrique (transfert au centre de l’ obésité).
1. WHO Fact sheet 311 uA. Obesity an overweight. 2014 (accessed 30. October 2014).
2. Collaboration NCDRF. Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 2016; 387(10026): 1377-96.
3. Collaboration NCDRF. Worldwide trends in body-mass index, underweight,
overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017; 390(10113): 2627-42.
4. Bluher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol 2019; 15(5): 288-98.
5. https://apps.who.int/iris/bitstream/handle/10665/353747/9789289057738-eng.pdf.
6. Malik VS, Willett WC, Hu FB. Global obesity: trends, risk factors and policy
implications. Nat Rev Endocrinol 2013; 9(1): 13-27.
7. Kivimaki M, Luukkonen R, Batty GD, et al. Body mass index and risk of dementia:
Analysis of individual-level data from 1.3 million individuals. Alzheimers Dement 2018; 14(5): 601-9.
8. Puhl RM, Brownell KD. Confronting and coping with weight stigma: an investigation of overweight and obese adults. Obesity (Silver Spring) 2006; 14(10): 1802-15.
9. Himmelstein MS, Puhl RM, Quinn DM. Intersectionality: An Understudied Framework for Addressing Weight Stigma. Am J Prev Med 2017; 53(4): 421-31.
10. Pearl RL, Puhl RM. Weight bias internalization and health: a systematic review. Obes Rev 2018; 19(8): 1141-63.
11. Himmelstein MS, Puhl RM, Pearl RL, Pinto AM, Foster GD. Coping with Weight Stigma Among Adults in a Commercial Weight Management Sample. Int J Behav Med 2020; 27(5): 576-90.
12. Puhl RM, Lessard LM, Himmelstein MS, Foster GD. The roles of experienced and internalized weight stigma in healthcare experiences: Perspectives of adults engaged in weight management across six countries. PLoS One 2021; 16(6): e0251566.
13. Albury C, Strain WD, Brocq SL, et al. The importance of language in engagement between health-care professionals and people living with obesity: a joint consensus statement. Lancet Diabetes Endocrinol 2020; 8(5): 447-55.
14. Puhl RM, Phelan SM, Nadglowski J, Kyle TK. Overcoming Weight Bias in the Management of Patients With Diabetes and Obesity. Clin Diabetes 2016; 34(1): 44-50.
15. https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/
a-healthy-lifestyle/body-mass-index-bmi.
16. Padwal RS, Pajewski NM, Allison DB, Sharma AM. Using the Edmonton obesity staging system to predict mortality in a population-representative cohort of
people with overweight and obesity. CMAJ 2011; 183(14): E1059-66.
17. Fujioka K, O’Neil PM, Davies M, et al. Early Weight Loss with Liraglutide 3.0 mg Predicts 1-Year Weight Loss and is Associated with Improvements in Clinical Markers. Obesity (Silver Spring) 2016; 24(11): 2278-88.
18. le Roux CW, Astrup A, Fujioka K, et al. 3 years of liraglutide versus placebo for type 2 diabetes risk reduction and weight management in individuals with prediabetes: a randomised, double-blind trial. Lancet 2017; 389(10077): 1399-409.
Pour les patients, il est décisif de savoir si le traitement de leurs problèmes de santé est pris en charge par l’ assurance-accidents ou par l’ assurance-maladie, car cette dernière prévoit une participation du patient aux frais engagés (franchise, quote-part). Cet article donne un aperçu des atteintes à la santé couvertes par l’assurance-accidents.
Due to the patient’s participation in the costs incurred as provided for in the health insurance (franchise, deductible), it is decisive whether the treatment of the health impairment is covered by the health insurance or the accident insurance. This article gives an overview of which health impairments are covered by accident insurance. Key Words: accident definition, bodily injury similar to that sustained in an accident, occupational disease, causality
La loi fédérale sur l’ assurance-accidents (LAA) prévoit que les prestations d’ assurance sont accordées conformément à cette loi en cas d’ accident professionnel, d’ accident non professionnel, de maladie professionnelle ou de lésions corporelles assimilées à un accident (art. 6 LAA). L’ assurance-maladie sociale accorde en revanche des prestations en cas de maladie, d’accident, pour autant qu’ aucune assurance-accidents n’en assume la prise en charge, et de maternité (art. 1a de la loi fédérale sur l’ assurance-maladie ; LAMal).
Accidents
La loi fédérale sur la partie générale du droit des assurances sociales (LPGA) définit quand il est présumé qu’il y a accident au sens du droit de l’ assurance-accidents. Toute atteinte dommageable, soudaine et involontaire, portée au corps humain par une cause extérieure extraordinaire qui compromet la santé physique, mentale ou psychique ou qui entraîne la mort, est considérée comme accident (art. 4 LPGA). En revanche, toute atteinte à la santé physique, mentale ou psychique qui n’ est pas due à un accident et qui exige un examen ou un traitement médical ou qui provoque une incapacité de travail, est réputée maladie (art. 3 al. 1 LPGA). La question de savoir si la notion d’ accident est remplie est une question juridique et doit donc être résolue par l’ application du droit; il ne s’ agit pas d’ une question médicale (1). Pour qu’ un accident soit reconnu par la loi, tous les critères énumérés doivent être remplis. La jurisprudence du Tribunal fédéral est particulièrement riche en ce qui concerne la question de l’ existence d’ un facteur extérieur extraordinaire (2). Dans le cadre du travail médical, il est souvent difficile de déterminer s’ il s’ agit d’ un accident au sens de la loi, de sorte que le terme d’ accident devrait être évité.
Il ressort de la définition de l’ accident qu’ il doit y avoir un certain lien entre l’ événement accidentel et l’ atteinte à la santé. Le Tribunal fédéral et la doctrine juridique définissent à cet égard que l’ assureur-accidents est obligé d’ allouer des prestations lorsqu’ il existe un lien de causalité naturelle et adéquate entre l’ événement accidentel et l’ atteinte à la santé (3).
La causalité naturelle permet d’ examiner le lien effectivement explicable entre la cause et les symptômes. Des aspects scientifiques et techniques sont pris en considération. Il s’ agit d’ une question médicale ou scientifique. A ce sujet le Tribunal fédéral retient que les causes au sens de la causalité naturelle sont toutes les circonstances sans lesquelles le dommage ne se serait pas produit du tout ou qu’il ne serait pas survenu de la même manière. Conformément à cette description, il n’ est pas nécessaire qu’ un accident soit la cause unique ou immédiate de l’atteinte à la santé pour que le lien de causalité naturelle soit établi ; il suffit que l’ événement dommageable, associé éventuellement à d’ autres facteurs, ait porté atteinte à l’ intégrité physique ou mentale de la personne assurée ; en d’ autres termes, l’ accident ne peut être supprimé sans que le trouble de la santé survenu ne disparaisse également (3).
Ce lien de causalité naturelle doit être établi avec le degré de preuve de la vraisemblance prépondérante. La simple possibilité d’ un lien ne suffit pas pour que l’ assureur-accidents soit tenu de fournir des prestations (3).
Selon le degré de preuve de la vraisemblance prépondérante, une preuve est considérée comme apportée lorsque des raisons objectives plaident en faveur de l’ exactitude de l’ allégation de fait, à tel point que d’ autres possibilités envisageables n’ entrent raisonnablement pas en ligne de compte de manière déterminante (4).
En d’ autres termes, le tribunal doit suivre l’ exposé des faits qu’ il considère comme le plus probable parmi tous les événements possibles (5).
Il convient de distinguer la causalité adéquate de la causalité négative. Celle-ci est examinée lorsque, à la suite de l’accident, aucune preuve organique n’a été apportée et que des troubles persistent malgré tout (6). A titre d’ exemple, on peut citer la persistance de douleurs cervicales sans preuve d’ une modification structurelle objectivable par une radiographie ou une IRM après un léger accident par l’ arrière. Par rapport à la causalité naturelle, il ne s’ agit pas d’ une théorie de la causalité logique, mais d’ une théorie de l’ imputation évaluative.
En conséquence, la question du lien de causalité adéquate, contrairement à la question du lien de causalité naturelle, est une question juridique (1).
Selon la jurisprudence, un événement est considéré comme la cause adéquate d’ un résultat, si, d’après le cours ordinaire des choses et l’expérience de la vie, le fait considéré était propre à entraîner un effet du genre de celui qui s’est produit, la survenance de ce résultat paraissant de manière générale favorisée par une telle circonstance (3). Le Tribunal fédéral a développé deux listes de critères différents que l’ application du droit doit examiner en fonction de la situation présente lorsqu’ il s’ agit de déterminer le lien de causalité adéquate (7).
Même si un assureur-accidents a affirmé son obligation de prestation, cela ne signifie pas dans tous les cas une prise en charge à vie des prestations. Un assureur-accidents doit par exemple suspendre ses prestations lorsqu’ il n’ y a plus de lien de causalité naturelle entre les troubles d’ une personne assurée et l’ événement accidentel ou que ce lien a disparu avec une probabilité prépondérante. Il convient de mentionner en particulier les constellations dans lesquelles l’ événement porte atteinte à une partie du corps déjà affectée par un état antérieur, souvent inconnu de la personne assurée (usure ou maladie). Pour que l’ obligation de verser des prestations soit illimitée dans le temps, il faut qu’ il y ait, à la suite de l’ accident, une aggravation durable ou déterminante d’ un état antérieur donné. Dès qu’ un état de santé atteint celui qui existait immédiatement avant l’ accident (statu quo ante) ou celui qui existerait même sans l’accident par suite d’un développement ordinaire (statu quo sine), l’ assureur-accidents doit suspendre ses prestations (8).
Une chute sur le genou après laquelle une gonarthrose est constatée, mais une rupture du ligament croisé antérieur est également diagnostiquée, peut servir d’ exemple d’ aggravation durable ou déterminante. Avec ou sans traitement chirurgical, il faut partir du principe que la rupture du ligament croisé antérieur a une influence négative sur l’ évolution de la gonarthrose. En revanche, on peut s’ attendre à une aggravation limitée dans le temps si une gonarthrose devient symptomatique à la suite d’une contusion sans lésion supplémentaire des ligaments ou du ménisque. Selon la sévérité de la contusion, l’ assurance-accidents est tenue de verser des prestations pendant quelques semaines à quelques mois. Il est dans la nature de l’ usure que des douleurs puissent apparaître indépendamment d’ un accident.
Lésions corporelles assimilées à un accident
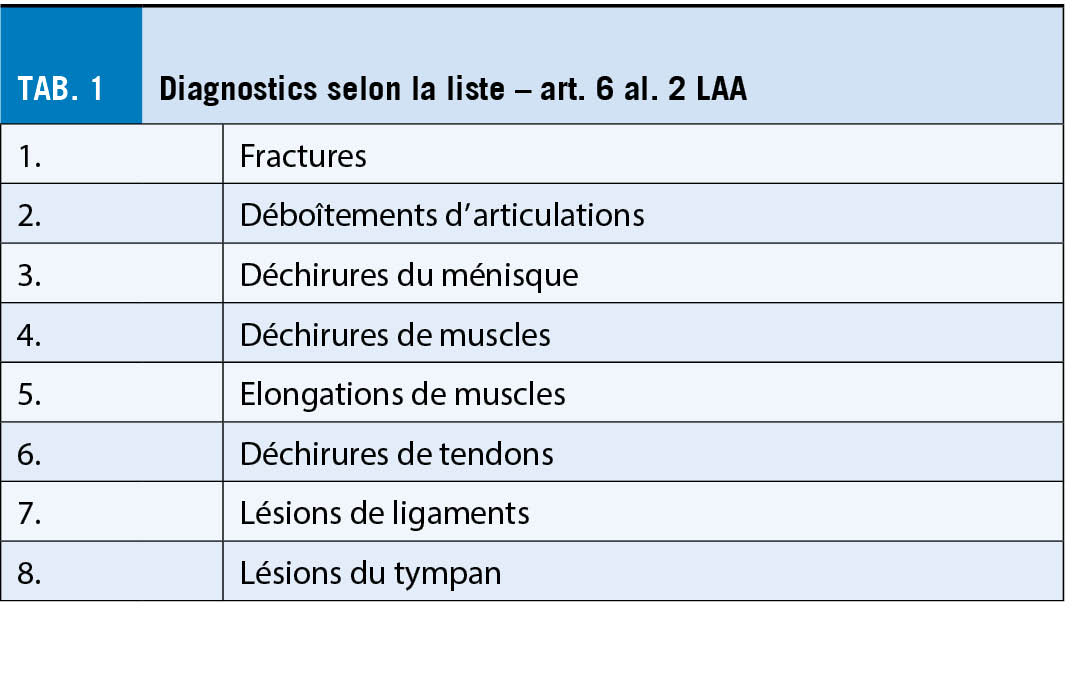
Outre l’ octroi de prestations d’ assurance en cas d’ accidents professionnels et non professionnels, l’ assurance-accidents fournit également ses prestations pour une liste exhaustive de huit diagnostics (tab. 1), pour autant qu’ ils ne soient pas dus principalement, c’ est-à-dire à plus de 50 % (9), à l’ usure ou à une maladie (art. 6 al. 2 LAA).
La condition préalable à une obligation de prestation est la présence de l’ un des diagnostics mentionnés. L’ examen de la pathogenèse de la pathologie à discuter dans le cas particulier est central dans l’ évaluation de la médecine des assurances. Si l’ examen de la pathogenèse conduit à la conclusion qu’ il existe une pathologie principalement due à l’ usure ou à une maladie, la compétence de l’ assureur-accidents doit être niée (10).
Maladie professionnelle
Enfin, l’ assureur-accidents est tenu de fournir des prestations en cas de maladie professionnelle. Dans ce contexte, il faut évaluer s’ il s’ agit d’ une maladie causée exclusivement ou de manière prépondérante, dans l’ activité professionnelle, par des substances nocives ou certains travaux (art. 9 al. 1 LAA). Le Conseil fédéral a établi une liste de ces substances et travaux ainsi que des maladies liées au travail (annexe 1 de l’ ordonnance sur l’ assurance-accidents ; OLAA).
Selon le Tribunal fédéral, les substances nocives ou certains travaux ne sont à l’ origine d’ une maladie de manière « prépondérante » que si elles pèsent plus lourd que toutes les autres causes impliquées, c’ est-à-dire si elles représentent plus de 50 % de l’ ensemble des causes. Par contre, la causalité « exclusive » signifie pratiquement 100 % de la part causale des substances nocives ou de certains travaux dans la maladie professionnelle (11). Mais d’ autres maladies dont il est prouvé qu’ elles ont été causées exclusivement ou de manière fortement prépondérante par l’ activité professionnelle sont également considérées comme des maladies professionnelles (art. 9 al. 2 LAA).
La maladie professionnelle doit être causée à 75 % au moins par l’ activité professionnelle. Ce sont surtout ces maladies, qui ne figurent pas sur la liste, qui donnent lieu à des discussions répétées dans la pratique quotidienne.
Pour qu’ une maladie professionnelle soit reconnue selon l’ art. 9 al. 2 LAA, il faut que le taux d’ incidence dans le groupe professionnel spécifique soit quatre fois plus élevé que celui de la population en général, afin de pouvoir affirmer le critère de la causalité exclusive ou nettement prépondérante de l’ activité professionnelle (12, 13).
Cet article est une traduction de « der informierte arzt » 06_2022
Copyright Aerzteverlag medinfo AG
Dr Josef Grab
MAS Médecine des assurances
EMBA HSG Insurance et Financial Services
Spécialiste en chirurgie, membre FMH
Suva
Fluhmattstrasse 1
6004 Lucerne
josef.grab@suva.ch
Nicole Pfrunder MLaw, avocate
Suva
Fluhmattstrasse 1
6004 Lucerne
nicole.pfrunder@suva.ch
Les auteurs n’ ont pas déclaré de conflits d’intérêts en rapport avec cet article.
◆ L’ assurance-accidents prend en charge les prestations en cas d’ accident, de lésions corporelles assimilées à un accident et de maladies professionnelles.
◆ L’ application du droit dépend, dans de nombreuses questions, d’ une évaluation médicale lors de l’ examen de l’ obligation de prestation. Il incombe notamment au corps médical de prendre position sur les questions de causalité naturelle.
◆ La notion d’ accident est définie dans la loi fédérale sur la partie générale du droit des assurances sociales La question de savoir si elle est remplie est une question juridique et doit donc être résolue par l’ application du droit. Il ne s’ agit pas d’ une question médicale.
◆ L’ affirmation de l’ obligation de prestation par un assureur-accidents ne signifie pas dans tous les cas une prise en charge des prestations à vie.
Jurisprudence et littérature :
1. Urteil des Bundesgerichts (BGer) 8C_298/2016 vom 30.11.2016 E. 5.2
2. zum ungewöhnlichen äusseren Faktor: BGE 134 V 72 E. 4.1
3. BGE 129 V 177 E. 3
4. BGE 140 III 610 E. 4.1
5. BGE 138 V 218 E. 6
6. BGE 140 V 356 E. 3.2
7. BGE 115 V 133 und BGE 134 V 109
8. Urteil des BGer 8C_589/2017 vom 21.2.2018 E. 3.1
9. BGE 146 V 51 E. 8.2.2.1
10. Koch H, Henseler S. Zur versicherungsmedizinischen Bewertung des Art. 6 Abs. 2 und der hiermit angegebenen Listendiagnosen im Bundesgesetz über die Unfallversicherung (UVG) der Schweiz. Der medizinische Sachverständige. 2020;116 (4):187-92.
11. BGE 117 V 354 E. 2a
12. BGE 116 V 136 E. 5c
13. Urteil des BGer 8C_746/2012 vom 29.10.2012 E. 5
L’ imagerie non-invasive du cœur joue un rôle clé dans la détection de la maladie coronarienne obstructive chez le patient symptomatique. La probabilité pré-test et des modificateurs de risque dirigent l’ algorithme diagnostic. La majorité des patients ayant une probabilité pré-test intermédiaire, le choix de la modalité non-invasive optimale revient au cardiologue et sera individualisé en fonction de certaines caractéristiques du patient ainsi que de la disponibilité et des expertise locales.
Non-invasive cardiac imaging plays a crucial role to diagnose chronic coronary syndrom in symptomatic patients. Pre-test probability combined with risk modificators guide the algorithm. The majority of patients fall in the range of intermediate pre-test probability and need non-invasive imaging. The optimal modality needs to be chosen by the cardiologists taking into account patient’ s characteristics as well as local disponibility and expertise. Key Words: Pre-test probability, risk modificators, functional cardiac imaging, myocardial ischemic burden
Introduction
La maladie coronarienne est une des causes majeures de morbidité-mortalité dans le monde et engendre des « coûts socio-économiques » importants. Afin de pouvoir détecter et traiter la maladie, on se sert de l’ imagerie cardiaque non-invasive, outil diagnostique puissant qui permet de diminuer de façon significative le nombre d’ examens invasifs. Suite à une mise à jour des recommandations de la société européenne de cardiologie (ESC) sur le syndrome coronarien chronique (1) et l’ imagerie non-invasive dans la maladie coronarienne (2), cet article a pour but d’ offrir au cardiologue un rappel de l’ algorithme diagnostique chez le patient symptomatique et de l’ aider à choisir la modalité optimale.
Quand une imagerie fonctionnelle est-elle indiquée ?
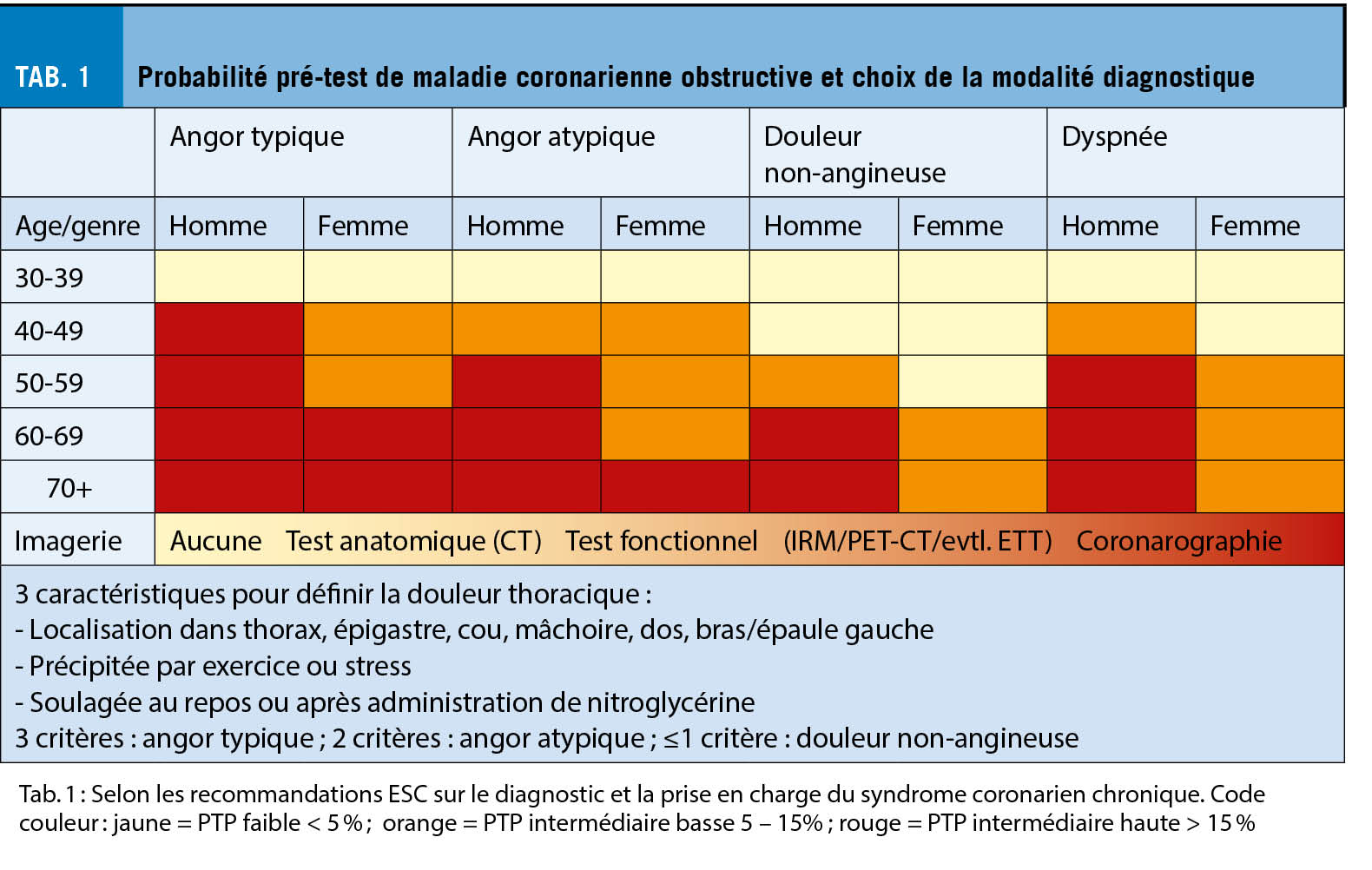
Les modèles de prédiction de la maladie coronarienne stable (MCS) obstructive ont été développés chez des personnes avec des douleurs thoraciques ou une dyspnée à l’ effort. De ce fait il est important d’ appliquer les outils de calcul de la probabilité pré-test (PPT) à ce groupe de patients. Malgré son ancienneté le diagramme de Diamond-Forrester (3) garde un rôle primordial dans l’ évaluation du risque et permet d’ orienter la prise en charge selon l’ âge, le sexe et le type de symptômes. Par contre, plusieurs études ont suggéré que la prévalence de la MCS obstructive était nettement plus basse qu’ initialement rapportée (4), raison pour laquelle les chiffres de la PPT ont été corrigés et le diagramme adapté (Diamond-Forrester modifié) (5). Le tableau 1 illustre la PPT et le choix de la modalité diagnostique proposée selon les recommandations de l’ ESC (1).
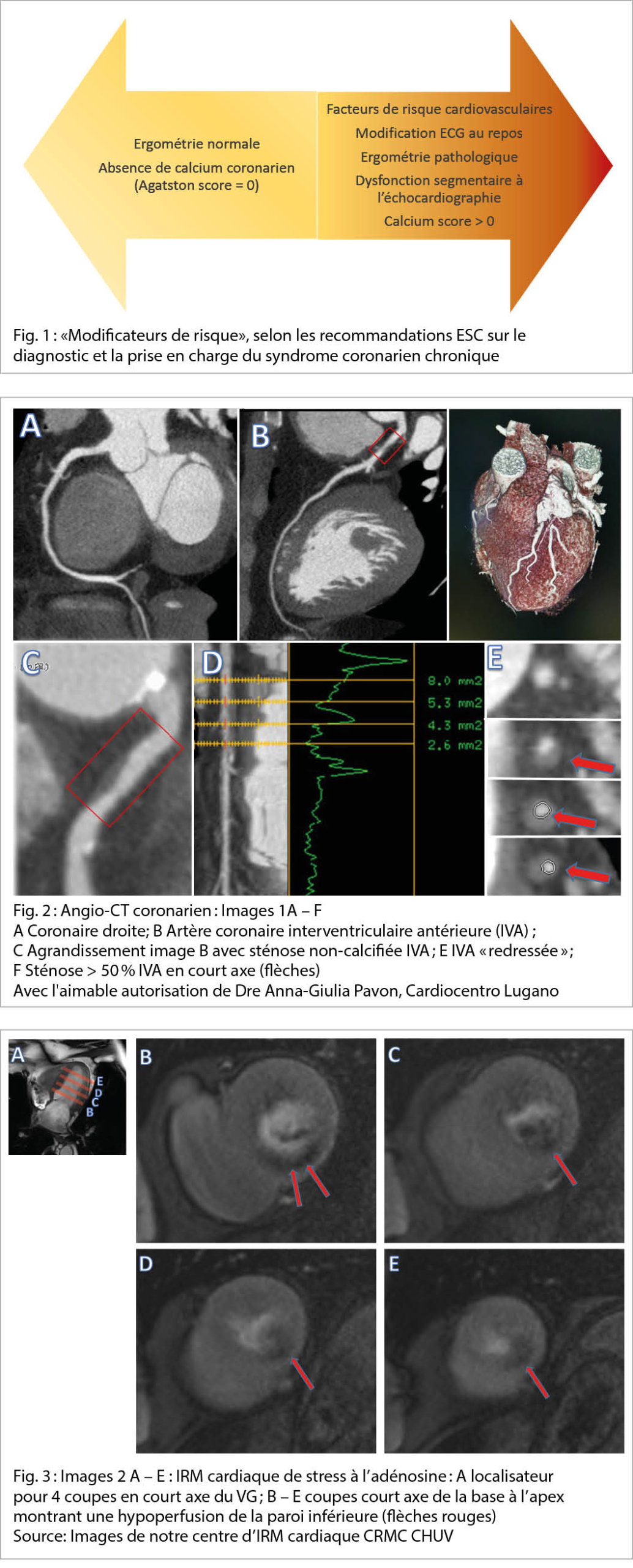
C’ est principalement dans le groupe de patients avec une PPT intermédiaire que le test fonctionnel permet de restratifier le risque et d’ en tirer une conclusion fiable. Pour une analyse plus fine, un nouveau concept dans les recommandations européennes de 2019 (1) consiste à évaluer des modificateurs de risque (MR) chez des patients avec une PPT intermédiaire basse (5 – 15 %). En présence d’ un des paramètres suivants, il est conseillé d’ aller à l’ imagerie non-invasive : présence de facteurs de risque cardiovasculaires (FRCV), ECG de repos ou d’ effort pathologique, ventricule gauche avec fonction systolique globale ou régionale anormale ou calcium score coronarien > 0 (cf. figure 1). Si aucun modificateur de risque n’ est présent ou que la PPT est très faible (< 5 %) une cause alternative aux symptômes doit être considérée. A l’ opposé devant une haute suspicion (angor typique au moindre effort ou rapidement évolutif), il est recommandé de procéder directement à une coronarographie. Dans ces deux extrêmes, les tests fonctionnels non-invasifs n’ ont pas de valeur ajoutée par rapport à l’ évaluation purement clinique. De toute manière, un ECG ainsi qu’ une échocardiographie transthoracique (ETT) au repos sont indiqués chez tout patient se présentant avec des symptômes à l’ effort et permettent soit d’ obtenir des arguments en faveur d’ une origine ischémique soit d’ orienter vers un diagnostic différentiel (bradycardie, dysfonction VG, péricardite, etc.).
Quel test choisir ?
Afin de pouvoir choisir la modalité la plus adaptée à un patient, il est important de comprendre les caractéristiques des tests disponibles détaillées ci-dessous. Ces tests sont repartis en imagerie anatomique et fonctionnelle. Pour chaque examen il existe certaines contre-indications ou des situations qui risquent de diminuer la qualité de l’ examen et donc sa valeur diagnostique.
Imagerie anatomique
CT cardiaque natif (score calcique coronarien selon Agatston) et angio-CT coronarien :
Le score calcique consiste en une mesure de la charge de calcium, reflétant l’ étendue de l’ athérosclérose de l’ arbre coronarien. L’ examen sert en premier lieu à exclure soit la présence d’ une maladie coronarienne (score calcique selon Agatston = 0) chez le patient asymptomatique avec des FRCV soit de MR chez le patient symptomatique avec une PPT intermédiaire basse. Vu l’ absence de visualisation des vaisseaux, le CT cardiaque est aujourd’ hui rarement effectué sans être couplé à un angio-CT coronarien.
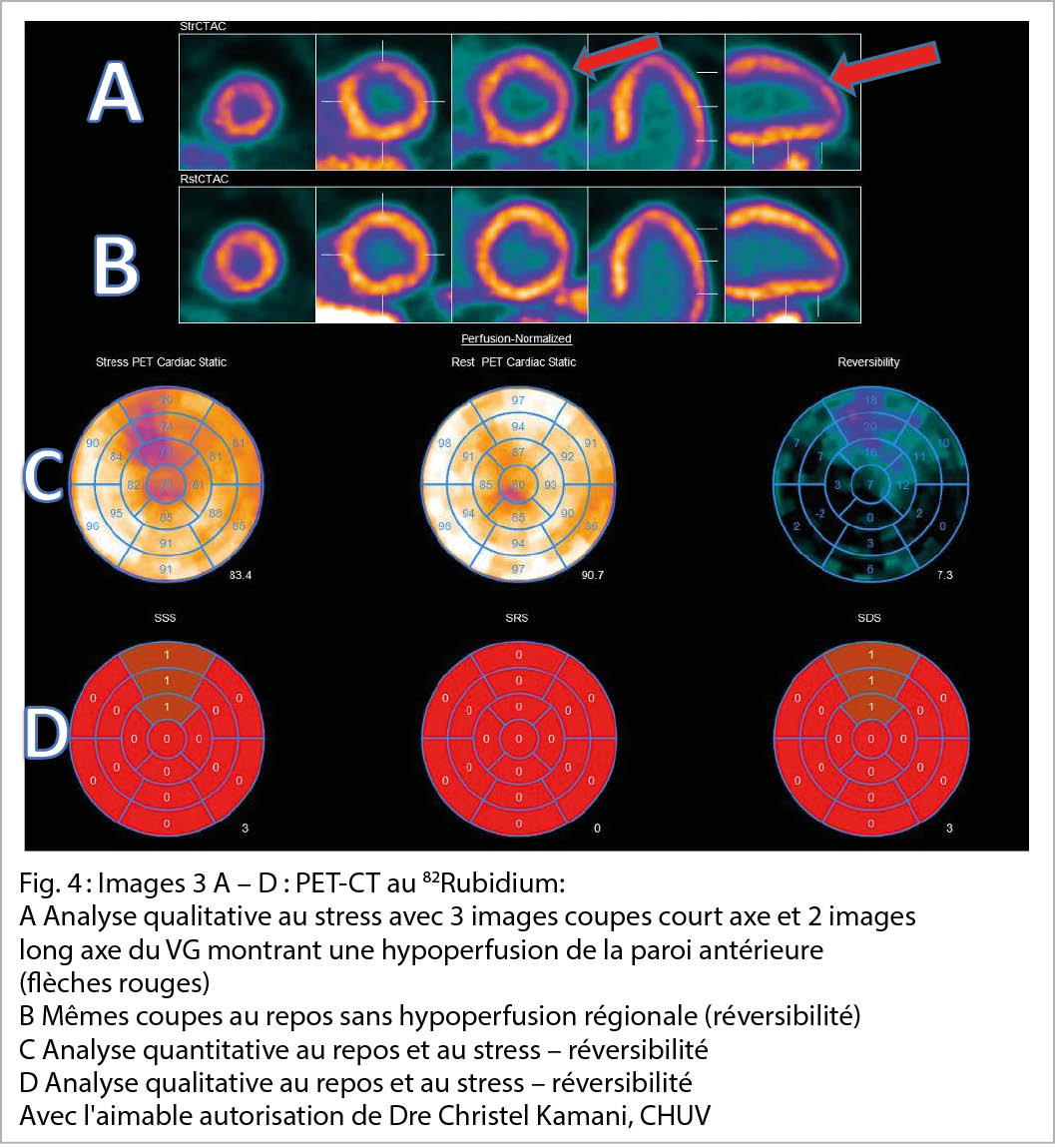
L’ angio-CT coronarien est un examen synchronisé au rythme cardiaque et met en évidence les artères coronariennes épicardiques par l’ injection de produit de contraste iodé sous réserve d’ une fréquence cardiaque contrôlée et régulière (< 70bpm). L’ absence de sténose >50 % dans une artère épicardique est corrélée à une excellente sensibilité pour exclure une sténose hémodynamiquement significative (6-8). Avec le but d’ améliorer la spécificité de l’ angio-CT coronarien, des études cliniques avec mesures du flux coronarien (FFR) sont en cours et s’ annoncent prometteuses et fiables en comparaison avec la FFR invasive. Le CT coronarien est également recommandé dans une situation de syndrome coronarien aigu à bas risque (dosage de troponines HS dans la norme, ECG normal ou modification aspécifique et non-dynamique) pour en exclure l’ origine coronarienne. L’ irradiation liée à cet examen est entre 1 et 10 mSv, ce qui est considérable surtout en cas d’ imagerie répétée.
Imagerie fonctionnelle
L’ imagerie fonctionnelle proprement dite a pour but de démontrer l’ ischémie myocardique en situation de stress pharmacologique ou physiologique. L’ IRM cardiaque et le PET-CT ont démontré la meilleure valeur prédictive en comparaison au gold standard de la coronarographie avec mesure par FFR. Ce n’ est pas surprenant puisque dans la cascade ischémique le défaut de perfusion survient avant l’ apparition de troubles de la cinétique segmentaire ou d’ anomalies à l’ ECG. Ces deux modalités prennent peu à peu la place des tests plus anciens (ergométrie, scintigraphie myocardique, échocardiographie de stress). Néanmoins l’ échocardiographie de stress garde une place importante parmi les cardiologues en raison de sa disponibilité et l’ apport diagnostique global sur la fonction et la structure du cœur de même que sur la capacité fonctionnelle du patient dans le cas d’ un effort physique. Pour permettre une valeur diagnostique suffisante dans la détection de la maladie coronarienne, l’ expertise de l’ opérateur et la sélection adéquate du patient sont indispensables. Toutefois, il n’ existe pas d’ étude comparant l’ ETT de stress à la mesure invasive de la FFR. La scintigraphie myocardique est à choisir seulement dans des cas où les autres modalités sont inaccessibles ou contre-indiquées car sa performance diagnostique est moindre, essentiellement due à la mauvaise résolution spatiale des images. Le choix de la modalité se fait premièrement en fonction de la PPT, mais aussi en prenant en compte les caractéristiques du patient donné (cf. figure 3), la disponibilité régionale et l’ expertise de chaque centre.
L’ IRM cardiaque de stress permet soit l’ évaluation de la cinétique segmentaire (et parfois la perfusion) sous dobutamine, soit l’ étude de la perfusion sous vasodilatateur (adénosine), cette dernière étant la plus fréquemment utilisée. De multiples études valident la valeur diagnostique et pronostique de l’ IRM cardiaque de stress (9-11). Sous dobutamine la cinétique segmentaire est évaluée de la même façon que pendant une échocardiographie de stress. Sous vasodilatation par adénosine on cherche à révéler les résistances au flux dans les coronaires épicardiques en faisant chuter et en équilibrant les résistances microvasculaires dans les différents territoires coronariens. En effet, 90 % des résistances globales se situent dans les petits vaisseaux et ces résistances baissent de manière physiologique en aval d’ une sténose significative afin d’ équilibrer la perfusion au repos. L’ analyse de la perfusion se fait la plupart de temps de manière qualitative sur 3 – 4 coupes du ventricule gauche en court axe. Des outils d’ intelligence artificielle s’ installent peu à peu et permettront une analyse quantitative systématique dans un future proche. Un avantage conséquent de l’ IRM est la détection d’ autres atteintes cardiaques (et extracardiaques) à l’ origine des symptômes du patient (péricardite, cardiomyopathie inflammatoire ou infiltrative, effets de masse, hernie hiatale, etc.). De plus, l’ examen permet d’ évaluer la viabilité d’ un territoire myocardique hypoperfusé et de guider la revascularisation. Par contre l’ acquisition des images est relativement longue avec une durée d’ examen entre 40 et 50 minutes et peut s’ avérer difficile chez des patients ayant des difficultés à rester couchés (douleurs, dyspnée, claustrophobie). Une autre modalité est également à choisir en cas de pacemaker/défibrillateur non-conditionnel, notamment avec sondes de pacemaker abandonnées ou épicardiques ou encore en cas d’ insuffisance rénale terminale. Dans certains centres, le patient asthmatique peut aujourd’ hui bénéficier d’ une vasodilatation par regadenoson (agoniste sélectif de l’ adénosine), qui a longtemps été considérée comme contre-indiquée chez les asthmatiques.
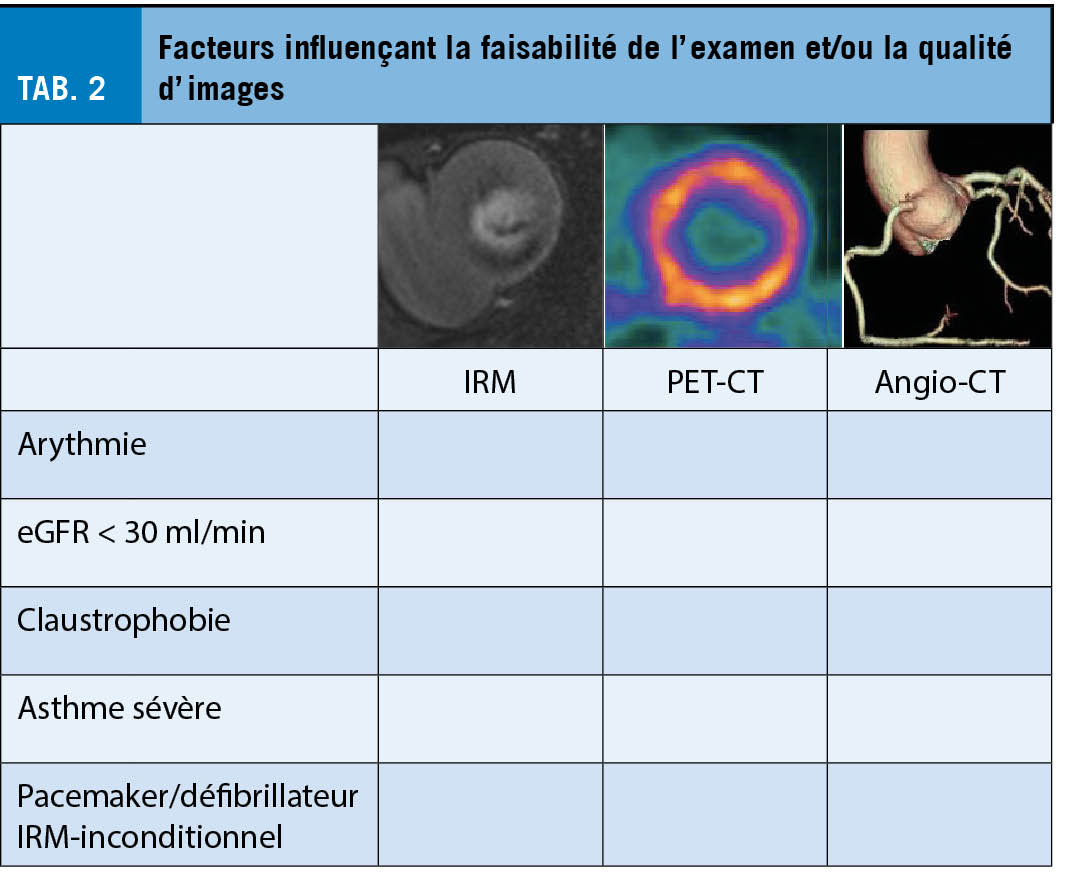
Le PET-CT cardiaque de perfusion est une modalité onéreuse et moins disponible que les autres, mais extrêmement sensible et spécifique dans le diagnostic de la MCS notamment grâce à l’ analyse quantitative de la perfusion myocardique (12, 13). Il est effectué sous vasodilatation (adénosine ou regadenoson) à l’ aide d’ un isotope (souvent 82Rubidium) avec des propriétés comparables au potassium. Son transport à l’ intérieur de la cellule requiert de l’ ATP et corrèle au flux coronarien. L’ analyse quantitative du flux permet un calcul de la réserve du flux et de la perfusion de chaque territoire coronarien et peut démontrer une hypoperfusion globale dans le contexte d’ une maladie tri-tronculaire ou d’ une atteinte micro-vasculaire. L’ irradiation reste un désavantage, notamment chez des gens jeunes qui doivent potentiellement subir de multiples examens radiologiques à venir. Une autre faiblesse de cette modalité est l’ impossibilité de rechercher une atteinte cardiaque structurelle ou une pathologie tissulaire (inflammation, cicatrice, fibrose). La différenciation entre nécrose myocardique et myocarde hibernant nécessite par ailleurs un examen supplémentaire avec un autre traceur (FDG). Une approche émergente très intéressante est l’ imagerie hybride angio-CT coronarien/PET-CT de perfusion, car elle permet de démontrer la maladie athérosclérotique ainsi que l’ ischémie et de guider la prévention primaire et secondaire.
Il a pu être démontré pour toutes les modalités présentées ci-dessus que l’ étendue de l’ ischémie corrèle avec le pronostic et identifie les patients qui bénéficient d’ une revascularisation précoce plutôt que d’ un traitement médicamenteux seul. Les seuils suivants ont été proposés :
Pour le PET-CT une ischémie de ≥ 10 % du myocarde du VG, pour l’ IRM cardiaque un défaut de perfusion touchant ≥ 2 sur 16 segments ou un trouble de la cinétique de ≥ 3 segments au stress sous dobutamine. Pour le CT coronarien, une maladie tritronculaire avec sténoses proximales ou une sténose significative de l’ IVA proximale ou du tronc commun.
Y a-t-il encore une place pour l’ imagerie fonctionnelle après l’ étude ISCHEMIA ?
L’ étude randomisée ISCHEMIA (14) publiée en 2020 a comparé une stratégie de revascularisation invasive à un traitement médicamenteux optimal chez 5179 patients avec une ischémie significative au test fonctionnel. Elle n’ a pas montré de bénéfice pour le traitement invasif après un suivi de 3.2 ans en termes de mortalité ou d’ événements cardio-vasculaires majeurs. Ce résultat a suscité des interrogations quant à l’ utilité des tests fonctionnels, mais il est important de relever, premièrement, qu’ il ne s’ agit pas d’ une étude qui était conçue pour étudier la valeur du test fonctionnel car il n’ y avait pas de groupe contrôle (sans test ou avec test négatif), deuxièmement que la majorité des patients n’ avaient pas de symptômes ou des symptômes légers. Par ailleurs, le test fonctionnel choisi était dans 49.6 % des cas la scintigraphie. Pour finir, tous les patients avec sténose de l’ IVA proximale ou du tronc commun étaient exclus de l’ étude, ce qui diminue la probabilité de mettre en évidence au test fonctionnel une ischémie sévère. Ces résultats sont donc à interpréter de façon prudente et ne devraient pas remettre en question l’ utilité des modalités d’ imagerie fonctionnelle modernes.
Deuxième impression de « info@cœur+vaisseau »
Copyright Aerzteverlag medinfo AG
Dre Sarah Hugelshofer
CHUV, Service de Cardiologie
Rue du Bugnon 46
1011 Lausanne
Sarah.Hugelshofer@chuv.ch
L’ auteure a déclaré n’ avoir aucun conflit d’ intérêts en rapport avec cet article.
◆ L’ imagerie fonctionnelle non-invasive est un outil puissant dans la détection et le suivi de la maladie coronarienne si le choix de la modalité est adapté au profil du patient et effectué par un opérateur expérimenté.
◆ En cas d’ une basse probabilité de maladie coronarienne, l’ angio-CT coronarien serait alors le premier choix afin d’ exclure une atteinte significative.
◆ L’ IRM et le PET-CT de perfusion sont des modalités optimales en cas de PPT intermédiaire. Le premier a l’ avantage de pouvoir mettre en évidence, en plus de l’ ischémie pronostique, des cicatrices ischémiques ou d’ autres atteintes myocardiques comme étiologie aux symptômes, tandis que le dernier permet une évaluation quantitative précise de la perfusion.
1. Maeder MT, Schoch OD, Kleiner R, Joerg L, Weilenmann D, Swiss Society For Knuuti J et al. : 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes : The Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). Eur Heart J 2019; 41:407-77
2. Edvardsen T et al. : Non-invasive imaging in coronary syndromes : recommendations of the European Association of Cardiovascular Imaging and the American Society of Echocardiography, in collaboration with the American Society of Nuclear Cardiology, Society of Cardiovascular Computed Tomography, and Society for Cardiovascular Magnetic Resonance. Eur Heart J 2021 ; 00 :1-28
3. Diamond GA, Forrester JS. Analysis of probability as an aid in the clinical diagnosis of coronary-artery disease. N Engl J Med 1979; 300:1350-58.
4. Genders TS et al. : Prediction model to estimate presence of coronary artery
disease : retrospective pooled analysis of existing cohorts. BMJ 2012 ; 344. e3485
5. Juarez-Orozco LE et al. : Impact of a decreasing pre-test probability on the performance of diagnostic tests for coronary artery disease. Eur Heart J Cardiovasc
Imaging 2019; 20:1998-207
6. Gueret P, Deux JF et al. Diagnostic performance of computed tomography coronary
angiography (from the prospective national multicenter multivendor EVASCAN study). Am J Cardiol 2013; 111:471-478.
7. Douglas PS, Hoffmann U, et a.. ; PROMISE Investigators. Outcomes of anatomical versus functional testing for coronary artery disease. N Engl J Med 2015; 372:1291-1300.
8. SCOT-HEART investigators. CT coronary angiography in patients with suspected angina due to coronary heart disease (SCOT-HEART): an open-label, parallelgroup, multicentre trial. Lancet 2015; 385:2383-2391.
9. Schwitter J, Wacker CM, et al. MRIMPACT II: magnetic resonance imaging for myocardial perfusion assessment in coronary artery disease trial: perfusion-cardiac magnetic resonance vs. single-photon emission computed tomography for the detection of coronary artery disease: a comparative multicentre, multivendor trial. Eur Heart J.(2013) 34:775–81.
10. Greenwood JP, Maredia N, et al. Cardiovascular magnetic resonance and singlephoton emission computed tomography for diagnosis of coronary heart disease (CE-MARC): a prospective trial. Lancet. (2012) 379:453–60.
11. Greenwood JP, Motwani M, et al. Comparison of cardiovascular magnetic resonance and single-photon emission computed tomography in women with suspected coronary artery disease from the Clinical Evaluation of Magnetic Resonance Imaging in Coronary Heart Disease (CE-MARC) trial. Circulation. (2014) 129: 1129–38.
12. Gewirtz H, Dilsizian V. Integration of quantitative positron emission tomography absolute myocardial blood flow measurements in the clinical management of
coronary artery disease. Circulation 2016;133:2180–96.
13. Schindler TH, Dilsizian V. PET-determined hyperemic myocardial blood flow: further progress to clinical application. J Am Coll Cardiol 2014;64:1476–8.
14. Maron DJ, Hochman JS, et al. Initial invasive or conservative strategy for stable coronary disease. N Engl J Med. (2020) 382:1395–407.
Les liens entre la douleur et la spiritualité ont été mis en évidence par les nouvelles connaissances issues des neurosciences. Les zones du cerveau intégrant les différentes modalités de la douleur et de la souffrance impliquent des circuits corticaux et sous-corticaux. La douleur et la spiritualité sont à la croisée des chemins et permettent de nouveaux développements de l’ accompagnement spirituel.
The links between pain and spirituality have been highlighted by new knowledge coming from neuroscience. The areas of the brain integrating the different modalities of pain and suffering involve cortical and sub-cortical circuits. Pain and spirituality are at the crossroad and allow further developments of spiritual care. Key Words: pain, spiritual distress, spiritual brain, logotherapy, spiritual care
Introduction
Que savons-nous aujourd’ hui de la douleur, ou plus précisément des douleurs, car elles apparaissent dorénavant sous des jours multiples, notamment avec les progrès des neurosciences. En effet, les douleurs occupent plusieurs régions du cerveau, tant cortical que sous-cortical. Elles peuvent être physiques, psychiques, psycho-sociales et plus récemment de nature existentielle et spirituelle.
Que savons-nous de la spiritualité, dans un siècle où déclinent les religions traditionnelles, au bénéfice d’ un essor important des spiritualités individuelles, de natures très variées. Car là aussi les neurosciences apportent un éclairage nouveau sur d’ anciennes questions. En effet, l’ étude du cerveau spirituel et religieux montre l’ importance des circuits mobilisés de manière cortico-sous corticale. Il apparaît dès lors que la spiritualité est un phénomène naturel et universel, une quête de lien et de sens, religieux ou non. En face, la religion est la réponse culturelle, traditionnelle, avec des rituels et de grands Médiateurs, impliquant plus ou moins de spiritualité.
C’ est pourquoi il est parfaitement légitime d’ investiguer à travers ces nouvelles connaissances les rapports entre douleurs et spiritualité, dans une perspective clinique intégrative. Le présent article fera le point sur cette interface, notamment quant au concept de détresse spirituelle et la réponse à y apporter : le spiritual care.
Douleurs
La douleur physique est bien connue, avec sa chaîne de transmission spécifique de la périphérie des tissus jusqu’ aux centres d’ intégration dans le cerveau. Les zones principales y sont bien sûr sensori-motrices dans les aires pariétales, mais aussi dans le cortex préfrontal pour sa prise de conscience et dans le cortex cingulaire antérieur pour l’ intégration affective en relation avec les régions sous-corticales du cerveau des émotions.
Cette anatomie fonctionnelle explique bien l’ intrication psychosomatique des syndromes douloureux. Les somatisations et les troubles somatoformes douloureux témoignent de cette complexité et donnent quotidiennement beaucoup de difficultés aux cliniciens.
La douleur psychique est fréquente en psychiatrie, apparaissant comme une forme grave du deuil et de la mélancolie. L’ imagerie fonctionnelle montre une mobilisation des zones sous-corticales. La douleur morale et le sentiment d’ indignité peuvent prendre un aspect délirant et provoquer une idéation suicidaire.
La douleur psycho-sociale a pu être démontrée plus récemment dans les situations d’ exclusion sociale, d’ isolement et de marginalisation. Ce sont alors les zones de la douleur relationnelle dans le cortex cingulaire antérieur qui prédominent.
Plus récemment, la recherche s’ est penchée sur les neurosciences de la spiritualité. Le cerveau spirituel est composé de très nombreux circuits cortico-sous-corticaux, responsables de donner du sens à l’ existence et une vision du monde qui donne du sens à la vie. Si le besoin de sens n’ est pas satisfait, on assiste alors à la détresse spirituelle, douleur existentielle. Ses symptômes sont la dépression, l’ agression et l’ addiction.
On retiendra donc que les douleurs utilisent les mêmes circuits et zones du cerveau, mais à des niveaux d’ organisation différents, en fonction de l’ organisation interne du sujet et de son rapport à l’ environnement, surtout relationnel et culturel.
Spiritualité
Dès l’ apparition des premiers humains et de la conscience réflexive, les premières communautés humaines doivent affronter l’ angoisse face aux mystères du monde, au mal et à la souffrance. Ce sera le rôle des chamanes de voir l’ invisible, par la transe, la conscience modifiée et les psychédéliques. Ils sont des passeurs de mondes, des guérisseurs à la fois prêtres et médecins. La médecine moderne a été fondée par Hippocrate, dont on oublie souvent qu’ il était prêtre d’ Asclépios, dieu guérisseur. Les Celtes pratiquaient la médecine des druides, et nous ont laissé leurs blouses blanches. Le Siècle des Lumières nous a propulsés dans le rationalisme, et la psychanalyse a contribué à désenchanter le monde.
Cependant, le besoin de sens continue d’ habiter nos patients et le regain d’ intérêt pour les spiritualités auquel nous assistons actuellement en témoigne.
Qu’ en dit la science ? De nombreuses études, principalement nord-américaines, ont démontré l’ impact favorable de la spiritualité sur la santé, tant pour la prévention que pour le rétablissement. Dans le champ des addictions, on retient l’ efficacité du mouvement des Alcooliques Anonymes, un mouvement spirituel mais non religieux. Fondé sur le lâcher-prise et à la remise à une Puissance supérieure, ses groupes constitués de millions d’ adhérents, AA reconstruit une sobriété existentielle et une solidarité exemplaire entre ses membres. De grandes études evidence based ont montré une efficacité équivalente, voire supérieure pour certains sous-groupes, aux principales formes de psychothérapies.
Ces dernières années, la recherche neuroscientifique a étudié les effets de la méditation sur le cerveau. Sous l’ impulsion de scientifiques d’ obédience bouddhiste, on a pu en montrer les effets bénéfiques sur la santé physique et mentale, par l’ acquisition d’ une plus grande souplesse aussi bien cognitive qu’ affective. En effet le sujet apprend à éloigner les préoccupations tant du passé que de l’ avenir et se concentre sur l’ instant présent, pouvant aller jusqu’ à un sentiment océanique ou à la vacuité. La pratique régulière de la méditation active la plasticité neuronale et provoque des changements durables dans la conscience et les comportements. La forme occidentalisée, la mindfulness, est maintenant d’ un usage courant en médecine et en psychiatrie.
La méditation a donc un effet unitif avec l’ univers, mais qu’ en est-il de la prière ? Les travaux d’ imagerie cérébrale ont montré des effets semblables à ceux de la méditation, à la différence importante que la prière recrute en plus le cerveau relationnel et du langage. En effet, le sujet s’ adresse à la Puissance supérieure telle que définie dans sa culture et installe un dialogue avec elle, que nous pouvons appeler un objet spirituel (ou virtuel). Dès lors il apparaît une instance régulatrice entre le sujet et lui-même, c’ est la fonction du Tiers, chère aux psychanalystes. Le sujet n’ est plus seul, il construit du sens.
Le sociologue médical Aaron Antonovsky a été déporté à Auschwitz. Il a observé la vie dans le camp et en a déduit que l’ être humain a un besoin de cohérence, définie comme la capacité de comprendre le monde, de gérer sa vie avec l’ aide de ce monde ou non, et de voir que ce qui arrive a du sens. La cohérence est le fondement de la salutogenèse, qui, à l’ inverse de la pathogenèse, cherche des attracteurs de sens et de santé dans le futur des patients.
Le neurologue et psychanalyste Viktor Frankl, contemporain de Freud, a également été déporté à Auschwitz avec toute sa famille. Seul survivant, il analyse la vie dans le camp et en tire des conclusions sur l’ humain et son besoin de sens. Pour Frankl, il existe un inconscient spirituel, et son refoulement produit une névrose de civilisation, caractérisée par le vide existentiel, dont les symptômes sont la dépression, l’ agression et l’ addiction. A son retour à Vienne, il pose les fondements d’ une thérapie par le sens, la logothérapie. Cette analyse existentielle offre au patient une réflexion thérapeutique sur ses raisons de vivre, par le moyen de l’ autodistanciation et de l’ autotranscendance.
Ces deux penseurs font partie des pionniers de ce qu’ on appelle dorénavant le spiritual care.
Spiritual care
L’ accompagnement religieux des malades a une longue tradition en Occident. Les différents rapports entre les Églises et les hôpitaux ont fortement évolué, notamment face au raccourcissement des durées de séjour, mais aussi face à la mondialisation et à la diversité spirituelle et religieuse. Dorénavant on parle d’ accompagnement spirituel ( l’ anglais « care » est plus large que le mot « soin ») et non plus d’ aumônerie. Les accompagnants spirituels (de toute origine confessionnelle) sont formés à accueillir toute demande au niveau de la question du sens. Il s’ agit d’ une évolution importante, favorable à l’ interdisciplinarité au lit du malade.
Des questionnaires brefs et faciles à administrer se sont développés en quelques questions investiguant la spiritualité des patients et peuvent intégrer l’ anamnèse (ex. : HOPE questionnaire). Des expériences d’ intégration des accompagnants spirituels sont en cours en Suisse romande dans les consultations multidisciplinaires de la douleur.
Conclusion
Dès lors, il est impératif dans une véritable médecine de la personne de tenir compte des trois ordres de la douleur et de la souffrance : physique, psychique et spirituelle.
Copyright Aerzteverlag medinfo AG
Pr Hon. Jacques Besson
Faculté de biologie et de médecine
Université de Lausanne
Rue du Bugnon 21
1005 Lausanne
L’ auteur n’ a pas déclaré de conflits d’ intérêts en rapport avec cet article.
Integrating Spirituality into Treatment. William R. Miller, APA Press, Washington 1999
Religion and Psychiatry ; Beyond Boundaries. Peter J. Verhagen et al,
Wiley-Blackwell, WPA, Oxford 2010
Principles of Neurotheology. Andrew B. Newberg, Ashgate, New York 2010
Spiritualité en milieu hospitalier. Pierre-Yves Brandt et Jacques Besson et al, Labor et Fides, Genève 2016
Addiction et spiritualité. Jacques Besson, Erès, Toulouse 2017
Clinique du sens. Elisabeth Ansen Zeder, Pierre-Yves Brandt et Jacques Besson, Archives contemporaines, Paris 2020