Aujourd’ hui, nous plongeons dans le monde complexe de l’ arthrose, une maladie articulaire débilitante qui touche des millions de personne s à travers le monde. Dans cette exploration, nous examinerons les injections articulaires, la thérapie physique et l’ utilisation du chondroïtine sulfate, en évaluant à la fois les risques et les avantages de ces approches.
La prévalence de l’ arthrose devrait continuer d’ augmenter à l’ échelle mondiale en raison du vieillissement de la population, de la hausse des taux d’ obésité et des lésions traumatiques. En 2019, environ 528 millions de personnes dans le monde vivaient avec l’ arthrose, un chiffre en hausse de 113% par rapport à 1990 (1). Avec une prévalence de 365 millions de personnes atteintes, le genou est l’ articulation la plus fréquemment touchée, suivi de la main et de la hanche (2). Parmi les personnes atteintes d’ arthrose, 344 millions présentent des niveaux de gravité (modérés ou graves) pour lesquels une réadaptation serait bénéfique (3). Néanmoins, l’ arthrose et les douleurs associées ne sont pas une conséquence inévitable du vieillissement.
Parmi les méthodes de soins qui peuvent être utilisées pour soulager les patients arthrosiques, ce numéro de la gazette traitera à la fois des méthodes plus invasives, telles que les injections articulaires, et des méthodes physiques pour soulager la douleur. Ensuite, nous aborderons les preuves sur l’ utilisation de la thérapie à la chondroïtine sulfate pour ralentir l’ évolution de l’ arthrose et réduire la douleur.
Les ponctions et infiltrations articulaires font partie des méthodes diagnostiques et thérapeutiques de plus en plus courantes, offrant une option prometteuse pour soulager la douleur et améliorer la fonctionnalité des articulations touchées par l’ arthrose. Cependant, il est crucial de peser attentivement les risques associés à ces injections, tels que les infections potentielles et les réactions allergiques. Les bénéfices, quant à eux, sont souvent significatifs, procurant un soulagement rapide et ciblé là où il est nécessaire. Les progrès dans les techniques d’ injection et les substances utilisées ouvrent la voie à des traitements plus personnalisés et efficaces.
La thérapie physique émerge également comme un pilier essentiel dans la gestion de l’ arthrose. En combinant des exercices spécifiques, le renforcement musculaire et des techniques de soulagement de la douleur, la thérapie physique offre une approche holistique pour améliorer la qualité de vie des patients. Elle favorise la mobilité articulaire, renforce les muscles environnants et offre une alternative non invasive aux traitements plus lourds.
Parmi les options de traitement, le chondroïtine sulfate se distingue comme un supplément suscitant un intérêt croissant. Ce composé, naturellement présent dans le cartilage, est souvent utilisé pour ralentir la progression de l’ arthrose et soulager les symptômes. Cependant, des études contradictoires existent quant à son efficacité, et il est important pour les patients de discuter de son utilisation avec leur professionnel de la santé.
En conclusion, face à l’ arthrose, il est primordial de combiner les approches médicales et non médicales pour offrir aux patients la meilleure qualité de vie possible. La recherche continue dans ce domaine promet des avancées significatives, ouvrant la voie à de nouveaux espoirs pour ceux qui souffrent de cette maladie débilitante.
Pre Patrizia D’ Amelio
Pre Patrizia D’ Amelio
Service de gériatrie et réadaptation gériatrique CHUV
Ch. de Mont-Paisible 16
1011 Lausanne
1. GBD 2019: Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019.
Lancet. 2020 Oct 17; 396(10258):1204-1222.
2. Long H, Liu Q, Yin H, Diao N, Zhang Y, Lin J et al. Prevalence trends of site-specific osteoarthritis from 1990 to 2019: Findings from the global burden of disease study 2019. Arthritis Rheumatol 2022; 74(7): 1172-1183.
3. Cieza A, Causey K, Kamenow K, Wulf Hansen S, Chatterji S, Vos T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020 Dec 19; 396(10267): 2006–2017.
Le refroidissement topique n’ est pas un moyen de protection lors de futures vagues de chaleur ?
En cas de vagues de chaleur, la mortalité augmente aussi en Suisse surtout chez les personnes âgées. Cela s’ explique entre autres par la réduction de la sensation de soif en fonction de l’ âge, l’ apport d’ eau sans électrolytes (avec risque d’ hyponatrémie) et l’ accès limité aux liquides (problèmes de mobilité). Dans une étude de petite taille, mais de grande qualité une moyenne d’ individus âgés de 72 ans ont été exposés pendant 6 heures à une température ambiante de 38 °C. Ensuite, aucun gradient de température n’ a été observé entre l’ environnement et la température centrale (qui, mesurée par voie rectale, se situait alors à 38 °C).
Des bains de pieds rafraîchissants et des compresses rafraîchissantes au niveau de la nuque (mesures également applicables en cas de coupure de courant due à la chaleur) n’ ont eu aucun effet par rapport au contrôle. En revanche, le groupe expérimental transpirait moins (buvait donc significativement moins et a développé une plus faible accélération du pouls. Les différences (taille de l’ effet) étaient toutefois très faibles et, selon les auteurs, cliniquement non pertinentes.
La surface corporelle à refroidir était probablement trop petite et la méthode n’ a pas eu d’ effet durable sur la convection de la température à la surface du corps.
JAMA 22023, doi:10.1001/jama.2023.24417, rédigé le 22.12.2023
Une fois de plus: on donne à ceux qui ont
La revue scientifique „Science“, ou plus précisément l’ American Association of Sciences qui l’ édite, verse chaque année 2,5 millions pour la percée scientifique de l’ année. Cette année, la percée récompensée est la classe des agonistes du récepteur GLP-1 dans leur action de réduction du poids. Deux des entreprises impliquées sont devenues en l’ espace d’ un an les entreprises les plus précieuses du monde, et les chercheurs et cliniciens qu’ elles ont typiquement soutenus financièrement se portaient déjà nettement mieux qu’ il y a un an avant la remise du prix …
Science 2023, https://www.science.org/boty2023 (vidéo et/ou podcast), rédigé le 22.12.2023
Le clozapine : trop peu prescrit ?
Le clozapine a été autorisé en 1988 pour le traitement de la psychose/schizophrénie et s’ est révélé particulièrement efficace dans les formes ne répondant pas aux autres traitements.
L’ absence d’ effets secondaires extrapyramidaux est également importante, et pas seulement en cas de maladies neurodégénératives (extrapyramidales) préexistantes. Il y a des raisons de penser que le clozapine a été abandonné en raison de la crainte de neutropénies, raison pour laquelle le clozapine a été retiré du marché temporairement. Ce sont surtout les contrôles réguliers de l’ hémogramme, initialement hebdomadaires, qui constituent un impondérable pour les cabinets psychiatriques. Les données suivantes pourraient changer cela: Le taux d’ incidence hebdomadaire le plus élevé de nouvelles neutropénies sérieuses (< 1000/ul) était de 0,128% après 9 semaines, le temps médian cumulé jusqu’ à l’ arrêt du clozapine étant de près de 18 semaines. Le taux d’ incidence des nouvelles neutropénies a ensuite diminué progressivement et n’ était plus que de 0,001% après 2 ans. Les auteurs recommandent – de manière bien compréhensible – des contrôles hebdomadaires de l’ hémogramme jusqu’ à 18 semaines après le début du traitement, puis une prolongation de l’ intervalle de contrôle à toutes les 4 semaines. 4 semaines et arrêt des contrôles après 2 ans.
The Lancet Psychiatry 2023, doi.org/10.1016/S2215-0366(23)00343-7, rédigé le27.12.2023
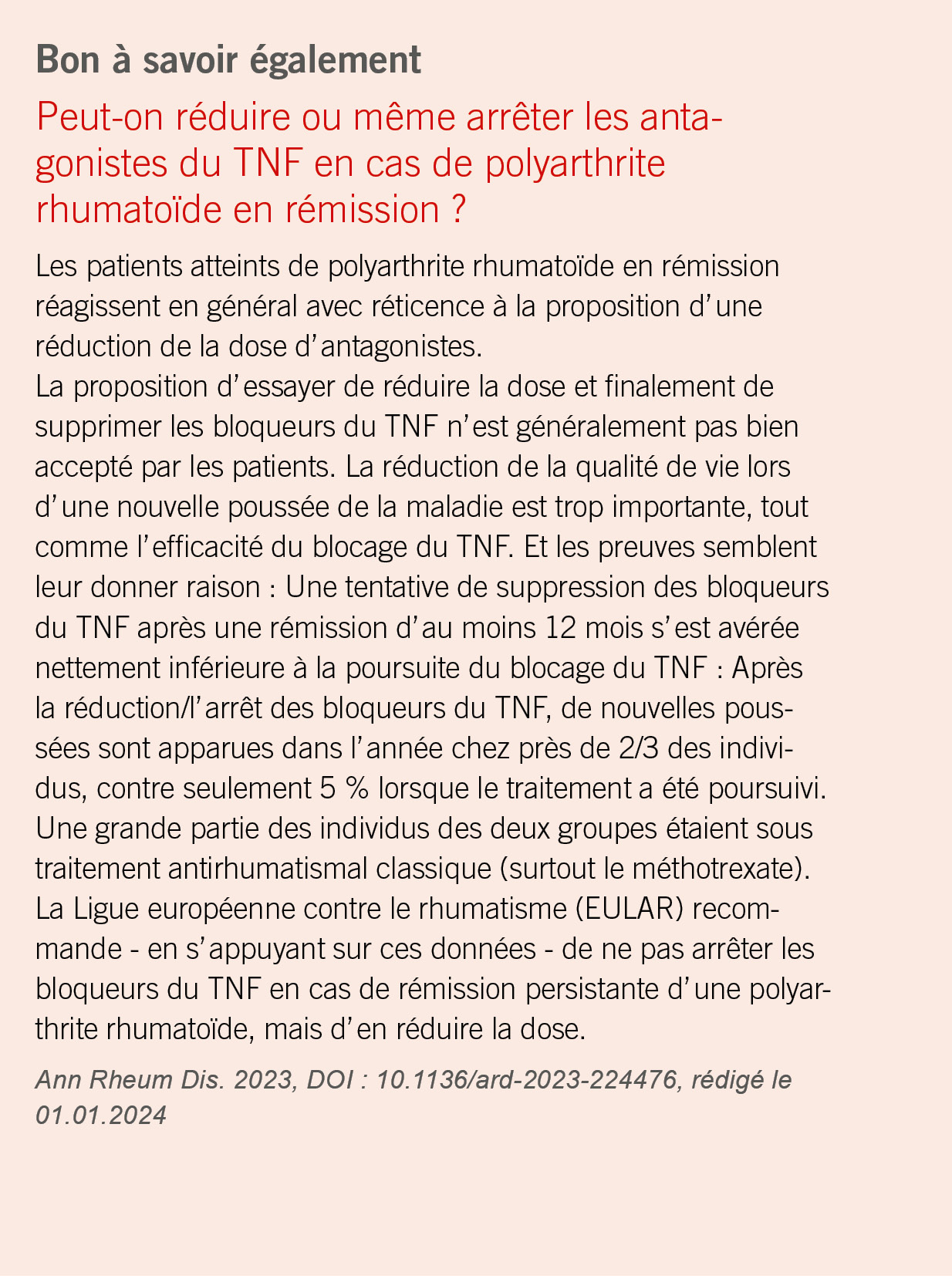
Bon à savoir également
Trouble anxieux concernant sa propre santé (hypocondrie) et pronostic
Dans votre cabinet, vous prenez presque certainement en charge des patients qui pensent souffrir d’ au moins une maladie organique ou/et qui surinterprètent les symptômes physiques dans le sens d’ un scénario catastrophe. Selon une cohorte suédoise de 4100 individus dits hypocondriaques, la mortalité (causes naturelles et non naturelles) a presque doublé (+ 86 %) en 25 ans par rapport à celle de 10 fois plus d’ individus (plus de 41 000) non hypocondriaques. Les causes de décès non naturels sont notamment les suicides (risque multiplié par 4), ce qui est probablement un signe de souffrance subjective, peut-être mal acceptée par l’ entourage, et de co-morbidités psychiatriques. La surmortalité naturelle, principalement due à des maladies cardiovasculaires et pulmonaires, est plus difficile à expliquer. Ce groupe de patients risque d’ être soumis à un nombre nettement plus élevé d’ examens médicaux, raison pour laquelle l’ interventionnisme médical peut être considéré comme une cause au moins partielle.
JAMA Psychiatry 2023, doi:10.1001/jamapsychiatry.2023.4744, redigé le 03.01.2024
Bientôt en application clinique?
Un espoir pour les individus atteints de glomérulonéphrite à IgA
Cette forme de glomérulonéphrite est de loin la plus fréquente des glomérulonéphrites. L’ âge principal de manifestation se situe chez les adolescents et les jeunes adultes. Elle est devenue une cause très importante d’ insuffisance rénale chronique dans le monde entier. L’ hypertension, la protéinurie et certains résultats histologiques de la biopsie rénale sont des facteurs prédictifs négatifs. Ceci est d’ autant plus vrai pour les patientes et les patients qui, malgré un traitement antiprotéinurique et antihypertenseur symptomatique (inhibiteur de l’ ECA ou bloqueur des récepteurs de l’ angiotensine ou antagoniste de l’ endothéline), continuent à présenter une protéinurie > 1gr/24h. Cette population a alors été traitée avec un anticorps monoclonal (sibeprenlimab) contre une protéine régulatrice de la formation des complexes immuns*. Avec une bonne tolérance, la protéinurie de ces individus prétraités a encore été réduite de moitié après 12 mois par rapport au placebo. Il s’ agit là de résultats encourageants dans le traitement d’ une maladie qui reste frustrante pour les personnes concernées et les médecins traitants. Il reste à savoir si la réduction de la protéinurie aura un effet sur le ralentissement de la progression de l’ insuffisance rénale. Il sera également intéressant de voir à l’ avenir si les inhibiteurs du SGLT-2 peuvent également exercer un effet protecteur important dans cette maladie.
*Les individus atteints de glomérulonéphrite à IgA produisent une molécule d’ IgA qui porte nettement moins de résidus de sucre (galactose) sur elle. Cette molécule d’ IgA pauvre en galactose est immunogène, c’ est-à-dire qu’ elle entraîne la formation d’ auto-anticorps puis de complexes immuns. Ceux-ci circulent, se déposent ensuite dans les glomérules et peuvent déclencher une glomérulonéphrite. L’ anticorps monoclonal testé inhibe l’ activation immunitaire qui conduit à la formation de complexes immuns.
NEJM 2024, DOI : 10.1056/NEJMoa2305635 et DOI : 10.1056/. NEJMe2312300, rédigé le 04.01.2024
L’ arthrose est une affection fréquente et invalidante chez le sujet âgé. Sa prise en charge repose principalement sur des mesures hygiéno-diétiques et non-pharmacologiques et peu d’ options thérapeutiques ont une balance risque/bénéfique favorable dans cette population. La chondroïtine est un anti-arthrosique d’ action lente largement utilisé dans le traitement symptomatique de l’ arthrose. L’ efficacité de cette substance est controversée, avec toutefois un possible bénéfice sur la diminution des douleurs arthrosiques et sur l’ amélioration de la qualité de vie qu’ il convient d’ évaluer au cas par cas.
Osteoarthritis is a frequent and disabling condition in older patients. Its management relies mainly on hygienic and dietary as well as non-pharmacological measures, and few therapeutic options have a favourable risk/benefit balance in this population. Chondroitin is a slow-acting anti-arthrosic widely used in the symptomatic treatment of osteoarthritis. The efficacy of this substance is controversial, although there may be a benefit in terms of reducing osteoarthritis pain and improving quality of life, which needs to be assessed on a case-by-case basis. Key words: arthrose, chondroïtine, traitement symptomatique, douleurs
L’ arthrose chez la personne âgée
L’ arthrose est une affection dégénérative des articulations qui provoque douleur, gonflement et raideur, affectant la capacité d’ une personne à se déplacer librement. Elle est plus courante au niveau des genoux, des hanches, de la colonne vertébrale et des mains. De nombreux facteurs peuvent contribuer au développement de l’ arthrose, notamment les antécédents de blessures articulaires ou de surutilisation des articulations, l’ âge avancé et le surpoids. Les personnes âgées sont particulièrement atteintes par cette maladie et les femmes plus que les hommes; en 2019, environ 528 millions de personnes dans le monde vivaient avec l’ arthrose, un chiffre en augmentation de 113 % par rapport à 1990 (1-2). La prévalence de cette maladie chronique devrait continuer d’ augmenter en raison du vieillissement de la population, de l’ augmentation de l’ obésité et des traumatismes.
L’ arthrose est une maladie difficile à traiter et il n’ existe que très peu d’ options thérapeutiques efficaces et sûres. Ces traitements sont les anti-inflammatoires non-stéroïdiens (AINS) déconseillés chez les personnes âgées, le paracétamol peu efficace dans les cas d’ arthrose sévère avec un risque de toxicité hépatique, et les opiacés parfois utilisés pour le traitement de l’ arthrose sévère qui comportent un risque iatrogénique marqué dans cette population. Présentée comme pouvant contribuer à la diminution de la douleur articulaire et à la réduction des limitations fonctionnelles, la chondroïtine (sulfate de chondroïtine) est largement rependue dans cette indication et de nombreux produits sont disponibles sur le marché. Mais quels sont les bénéfices et les risques de cette substance?
La chondroïtine: quelques aspects pharmacologiques
La chondroïtine est un mucopolysaccharide, extrait purifié de tissus cartilagineux d’ origine animale. Elle est naturellement présente dans tous les tissus conjonctifs et cartilagineux de notre organisme dont elle assure, entre autres, leur structure et leur élasticité en lien avec sa capacité marquée à fixer l’ eau. La chondroïtine fait partie de la classe des Anti-Arthrosiques Symptomatiques d’ Action Lente (AASAL) qui comprend également les glucosamines, la diacerhéine et les insaponifiables (d’ avocat ou de soja). La chondroïtine est disponible sur prescription médicale, en OTC et comme complément alimentaire. En Suisse, elle est inscrite dans la liste de spécialité et remboursée par l’ assurance de base.
L’ effet de la chondroïtine dans les pathologies ostéoarticulaires est attribué à son activité inhibitrice de la synthèse de composés pro-inflammatoires et de prostaglandines et stimulatrice de la synthèse de protéoglycanes. Par ailleurs, des études in vitro suggèrent une diminution de l’ activité catabolique des chondrocytes et la synthèse d’ enzymes protéolytiques susceptibles d’ endommager la matrice cartilagineuse et de provoquer la mort des chondrocytes. En outre, elle joue un rôle dans la formation de nouveaux os, cartilages et tendons, et maintient l’ intégrité structurelle des tissus (3).
D’ un point de vue pharmacocinétique, la chondroïtine est absorbée avec une biodisponibilité de 10 à 20%. Elle n’ est pas métabolisée par les cytochromes P450, mais rapidement hydrolysée en mono-, oligo- et polysaccharides dans le foie, ce qui limite le risque d’ interaction médicamenteuse. Elle s’ accumule dans les tissus articulaires, avec un état d’ équilibre atteint après 3-4 jours. Le délai d’ action est retardé et commence à apparaître au bout d’ un mois se confirmant à 2 mois et il faut environ 3-6 mois pour obtenir l’ effet maximal. La chondroïtine a un effet rémanent qui se poursuit jusqu’ à 2 mois après l’ arrêt du traitement s’ il a été pris au moins deux bimestres consécutifs (3-4).
La chondroïtine est bien tolérée et ne semble pas présenter de problèmes de sécurité majeurs. Toutefois, une récente infovigilance du dispositif de nutrivigilance de l’ Agence nationale de sécurité sanitaire de l’ alimentation française a mis en évidence un risque associé à la consommation de produits contenant de la chondroïtine et/ou de la glucosamine. Les effets indésirables principaux reportés étaient gastroentérologiques, hématologiques (purpura thrombopénique et perturbation de l’ INR), hépatiques et dermatologiques (5). Les effets indésirables de type gastro-intestinaux peuvent être réduits en prenant le médicament pendant le repas. Il convient de noter de rares cas d’ oedèmes et/ou de rétention hydrique chez des patients insuffisants rénaux et cardiaques.
Quelles évidences d’ efficacité?
De nombreuses recherches ont évalué l’ efficacité de la glucosamine et de la chondroïtine, séparément ou ensemble, dans le soulagement de la douleur et l’ amélioration de la fonction articulaire, dont les résultats sont contradictoires. Les recommandations de Osteoarthritis Research Society International (OARSI) indiquent un bénéfice incertain dans la réduction de la douleur de l’ arthrose du genou, sans effet sur la maladie (6). Un rapport d’ expert publié par la Société Suisse de Rhumatologie justifie l’ utilisation de la chondroïtine et/ou de la glucosamine en l’ absence d’ alternative médicamenteuse avec un meilleur rapport bénéfice/risque (7).
Une large métanalyse évaluant l’ efficacité de la chondroïtine dans l’ ostéoarthrose (majoritairement gonarthrose, plus rarement coxarthrose et arthrose de la main) rapporte un possible bénéfice de cette molécule sur la base de 4962 participants traités par chondroïtine versus 4148 participants traités par un placebo ou d’ autres comparateurs actifs (anti-inflammatoires non stéroïdiens, analgésiques, opioïdes, glucosamine ou d’ autres médicaments à base d’ herbes médicinales) sur une durée de 1 mois à 3 ans (8). Les critères d’ évaluation étaient la douleur, la raideur et la fonction physique (échelle numérique/visuelle analogique ou WOMAC The Western Ontario and McMaster Universities Arthritis Index), l’ indice algo-fonctionnel de Lequesne (indice de douleur, fonction physique et qualité de vie) et la réduction de la largeur minimale de l’ espace articulaire (radiographie).
Les résultats de cette métanalyse suggèrent une douleur 10% inférieure (intervalle de confiance à 95 % (IC95%), 15% à 6%) chez les patients traités par chondroïtine jusqu’ à 6 mois vs. le comparateur avec un nombre nécessaire à traiter de 5 (IC95% 3 à 8). Dans les essais basés > 6 mois de traitement, la différence était non significative (9% IC95% de 18 % à 0 %). En se basant sur l’ échelle de WOMAC, une réduction de 20% de la douleur au genou a été obtenue par 53% des patients du groupe chondroïtine contre 47% du groupe placebo, soit une différence de risque absolu de 6% (IC95% 1% à 11%). Basé sur le critère composite de Lequesne chez les patients traités jusqu’ à 6 mois, la différence de risque absolu était de 8% (IC95% 12 % à 5 %). Aucune différence statistiquement significative de fonctionnalité et de la plupart des autres mesures cliniques et radiographiques n’ a été observée. Cette métanalyse n’ a pas rapporté de différences statistiquement significatives dans le nombre d’ événements indésirables, d’ abandons pour cause d’ événements indésirables par rapport au placebo ou à un contrôle actif. Il est toutefois à relever que les effets indésirables sérieux étaient inférieurs dans le groupe chondroïtine que dans les groupes des comparateurs. En 2018, les résultats d’ une autre métanalyse évaluant l’ efficacité de la chondroïtine vs placebo, seule ou en association, sur l’ ostéoarthrite symptomatique du genou de patients traités pendant au moins un mois confirment une diminution de 7.1 % (IC95 % 11,0 % à 3,42 %) de la douleur, sans différence significative sur l’ index WOMAC (-1,40 %; IC95 % -4,5 % à 1,71 %)(9).
En résumé, les études indiquent une légère réduction de la douleur à court terme (< 6 mois) par la prise de chondroïtine seule ou en association, ainsi qu’ une possible légère amélioration de la qualité de vie, ayant toutefois à l’ esprit le faible niveau de preuves, le risque de biais élevé et la forte hétérogénéité des études. L’ intérêt thérapeutique de la chondroïtine pourrait résider dans la substitution aux AINS et permettre l’ économie de l’ utilisation chronique de ces derniers, évitant ainsi les complications liées à leur emploi chez le patient âgé, sans toutefois que cet intérêt ait été démontré par des données probantes.
Prise en charge globale de l’ arthrose
La prise en charge de l’ arthrose repose avant tout sur des mesures hygiéno-diététiques, comprenant la perte de poids, des programmes d’ exercices pour soulager la douleur et augmenter les capacités fonctionnelles, la kinésithérapie, le port d’ orthèses, et le recours aux cannes. Bien que l’ efficacité de la chondroïtine soit controversée selon les critères de l’ « evidenced-based medicine », un bénéfice fonctionnel et sur la douleur pourrait être perçu chez certains patients. L’ effet thérapeutique se manifestant après 1 à 2 mois de traitement, la chondroïtine devrait être prescrite en cures longues de 2 à 6 mois pour maximiser l’ efficacité et interrompue si aucune amélioration symptomatique n’ était apparente dans les 6 mois (10).
Copyright Aerzteverlag medinfo AG
PreChantal Csajka
Centre de Recherche et d’ Innovation en Sciences Pharmaceutiques
cliniques Centre Hospitalier Universitaire et Université de Lausanne
Suisse Rue du Bugnon 19
1011 Lausanne
Chantal.Csajka@chuv.ch
Sophia Hannou
Service de Pharmacie, Centre Hospitalier Universitaire Vaudois
et Université de Lausanne, Lausanne
Pre Patrizia D’ Amelio
Service de gériatrie et réadaptation gériatrique CHUV
Ch. de Mont-Paisible 16
1011 Lausanne
Les auteurs n’ ont pas déclaré de conflits d’ intérêts en rapport avec cet article.
◆ L’ arthrose est une maladie fréquente et invalidante chez le patient âgé et il n’ existe que très peu d’ options thérapeutiques efficaces et sûres.
◆ Le bénéfice clinique de la chondroïtine dans l’ arthrose, utilisé seul ou en combinaison avec la glucosamine, reste controversé, avec un effet faible principalement sur les douleurs.
◆ Le bénéfice du traitement apparait à 2 mois et une réévaluation de la balance risque/bénéfice à 6 mois s’ impose pour éviter la poursuite inutile du traitement.
◆ L’ épargne en anti-inflammatoire non-stéroïdien n’ est en pratique pas confirmé par des données probantes.
1. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020 Oct 17;396(10258):1204-1222.
2. Long H, Liu Q, Yin H, Diao N, Zhang Y, Lin J et al. Prevalence trends of site-specific osteoarthritis from 1990 to 2019: Findings from the global burden of disease study 2019. Arthritis Rheumatol 2022; 74(7): 1172-1183.
3. Henrotin Y, Mathy M, Sanchez C, Lambert C: Chondroitin sulfate in the treatment of osteoarthritis: from in vitro studies to clinical recommendations. Ther Adv Musculoskelet Dis. 2010 Dec;2(6):335-48.
4. Knox C, Wilson M, Klinger CM, et al. DrugBank 6.0: the DrugBank Knowledgebase for 2024. Nucleic Acids Res. 2024 Jan 5;52(D1):D1265-D1275.
5. Vidal. Compléments alimentaires à visée articulaire : la glucosamine et la chondroïtine sulfate potentiellement à risquehttps://www.vidal.fr/actualites/23171-complements-alimentaires-a-visee-articulaire-la-glucosamine-et-la-chondroitine-sulfate-potentiellement-a-risque.html [cité le 28.02.2024]
6. McAlindon T, Bannuru R, Sullivan M, Arden N, Berenbaum F, Bierma-Zeinstra S, Hawker Henrotin, G, Hunter D, Kawaguchi H, Kwoh K, Lohmander S, Rannou F Roos E, Underwood M. OARSI guidelines for the non-surgical management of knee Osteoarthritis. Osteoarthritis and Cartilage 22 (2014) 363e388
7. Société Suisse de Rhumatologie. https://www.rheuma-net.ch/fr/informations-d-experts [cité le 28.02.2024]
8. Singh JA, Noorbaloochi S, MacDonald R, Maxwell LJ. Chondroitin for osteoarthritis. Cochrane Database of Systematic Reviews 2015 Jan 28;1(1):CD005614.
9. Simental-Mendía M, Sánchez-García A, Vilchez-Cavazos F, Acosta-Olivo C, Pena-Martinez V, Simental-Mendia L. Effect of glucosamine and chondroitin sulfate in symptomatic knee steoarthritis: a systematic review and meta-analysis of randomized placebo-controlled trials. Rheumatol Int 38, 1413–1428 (2018).
10. Romain Thieubau. Proposition d’ outils à l’ attention du pharmacien d’ officine dans le cadre de la prise en charge des douleurs arthrosiques du sujet âgé. Sciences pharmaceutiques. 2021. dumas-03329132
L’ arthrose entraîne des douleurs sévères, affectant la mobilité et la qualité de vie, surtout chez les plus de 55 ans, en particulier les femmes. La physiothérapie, axée sur le développement et la préservation des capacités fonctionnelles, est cruciale pour la gestion de la douleur arthrosique. Cet article explore les interventions physiques proposées en physiothérapie dans le cadre des douleurs liées à l’arthrose, mettant en évidence leur efficacité. La douleur est complexe et nécessite une approche individualisée. L’ exercice, incluant renforcement musculaire, endurance, souplesse et équilibre, offre des bénéfices certains. Un programme structuré adapté à l’ individu peut maximiser ces effets. A l’inverse, massages et électrostimulation ne sont pas recommandés. En conclusion, un mode de vie actif et des exercices adaptés jouent un rôle crucial dans la gestion de la douleur et l’ amélioration de la qualité de vie des personnes atteintes d’ arthrose.
Osteoarthritis causes severe pain, impacting mobility and quality of life, especially in those over 55, particularly women. Physiotherapy, focused on developing and preserving functional capacities, is crucial for managing arthritic pain. This article explores physical interventions, highlighting their effectiveness. The complex nature of pain requires an individualized approach. Exercise, including muscle strengthening, endurance, flexibility, and balance, provides benefits. A structured program tailored to the individual can maximize these effects. However, massages and electrostimulation are not recommended. In conclusion, an active lifestyle and tailored exercises play a crucial role in managing pain and improving the quality of life for people with osteoarthritis.
Introduction
L’ arthrose est une affection dégénérative des articulations. Elle touche l’ ensemble des articulations, y compris les tissus qui l’ entourent. Elle apparaît le plus souvent aux genoux (85%), aux hanches, à la colonne vertébrale et aux mains (1). Prévalente chez les personnes de plus de 55 ans (73%), elle touche davantage les femmes (60%) (1). L’ incidence de l’ arthrose du genou et de la hanche augmente constamment avec l’ âge pour les deux sexes, tandis que le risque d’ arthrose des mains atteint son pic autour de la ménopause chez les femmes (1).
Cette condition engendre des douleurs, des gonflements et des raideurs, entraînant une altération de la capacité d’ une personne à se déplacer librement (1). Parmi les symptômes, la douleur est souvent perçue comme le plus handicapant par les patients (2). L’ arthrose est invalidante et constitue une charge de santé considérable et croissante, avec des répercussions significatives sur les individus concernés en termes de handicap et de qualité de vie (2). En raison des effets cumulés du vieillissement de la population mondiale, de l’ augmentation de l’ obésité, de la multiplication des blessures articulaires et de l’ inactivité, ce syndrome déjà lourd prend une ampleur croissante (2).
La physiothérapie est une thérapie délivrée par des physiothérapeutes à des personnes et à des populations pour développer, préserver et restaurer un maximum de mouvements et de capacités fonctionnelles tout au long de la vie. La physiothérapie est indiquée lorsque le mouvement et la fonction sont menacés, par exemple par le vieillissement, une ou plusieurs blessures, ou encore des douleurs et diverses pathologies. (3).
Si la physiothérapie est traditionnellement prescrite dans le cadre de l’ arthrose et de ses douleurs, les patients se voient régulièrement proposer des traitements à l’ efficacité discutable. Cet article abordera les différentes mesures physiques pratiquées dans ce cadre, et leur efficacité.
La douleur
La douleur liée à l’ arthrose présente une importante hétérogénéité, variant d’ un individu à l’ autre et à différentes phases de la maladie. Cette complexité rend l’ évaluation de cette douleur particulièrement délicate. Traditionnellement, la douleur est considérée comme nociceptive, résultant d’ une charge anormale sur une articulation endommagée (4). Cependant, certains patients présentent un composant inflammatoire dans leur expérience douloureuse. Des recherches récentes indiquent également une prévalence significative de la douleur neuropathique chez les personnes souffrant d’ arthrose du genou ou de la hanche, atteignant 23% (4). Contrairement à la douleur nociceptive, déclenchée par des dommages réels aux tissus ou des stimuli potentiellement dommageables pour les tissus, la douleur neuropathique découle des lésions du système nerveux lui-même. Une meilleure compréhension de ces composants multifactoriels de la douleur liée à l’ arthrose est essentielle pour une meilleure prise en charge (4).
La douleur liée à l’ arthrose du genou est généralement intermittente et principalement liée au poids (mécanique) (2). Souvent, la douleur intermittente est prévisible, mais lorsqu’ elle devient plus intense, plus fréquente ou imprévisible, les patients la catégorisent plus souvent comme inacceptable. Le concept et la compréhension des crises, appelées „flare-ups“, évoluent et sont désormais considérés comme plus larges qu’ une simple exacerbation de la douleur (2). Contrairement aux idées reçues, les images traditionnelles par rayons X et IRM montrent seulement des associations modérées entre l’ arthrose structurelle et la présence de douleur chez les individus affectés (2).
Bien que l’ arthrose soit un défi médical important, un traitement modifiant la maladie n’ est pas encore disponible. Le traitement antalgique médicamenteux (paracétamol et AINS) reste le traitement de prédilection de la douleur (2). Les infiltrations restent réservées aux échecs médicamenteux par voie orale (2). Il convient de noter que la chirurgie est envisagée en dernier recours, soulignant ainsi l’ importance d’ explorer des options moins invasives avant de recourir à des interventions plus lourdes.
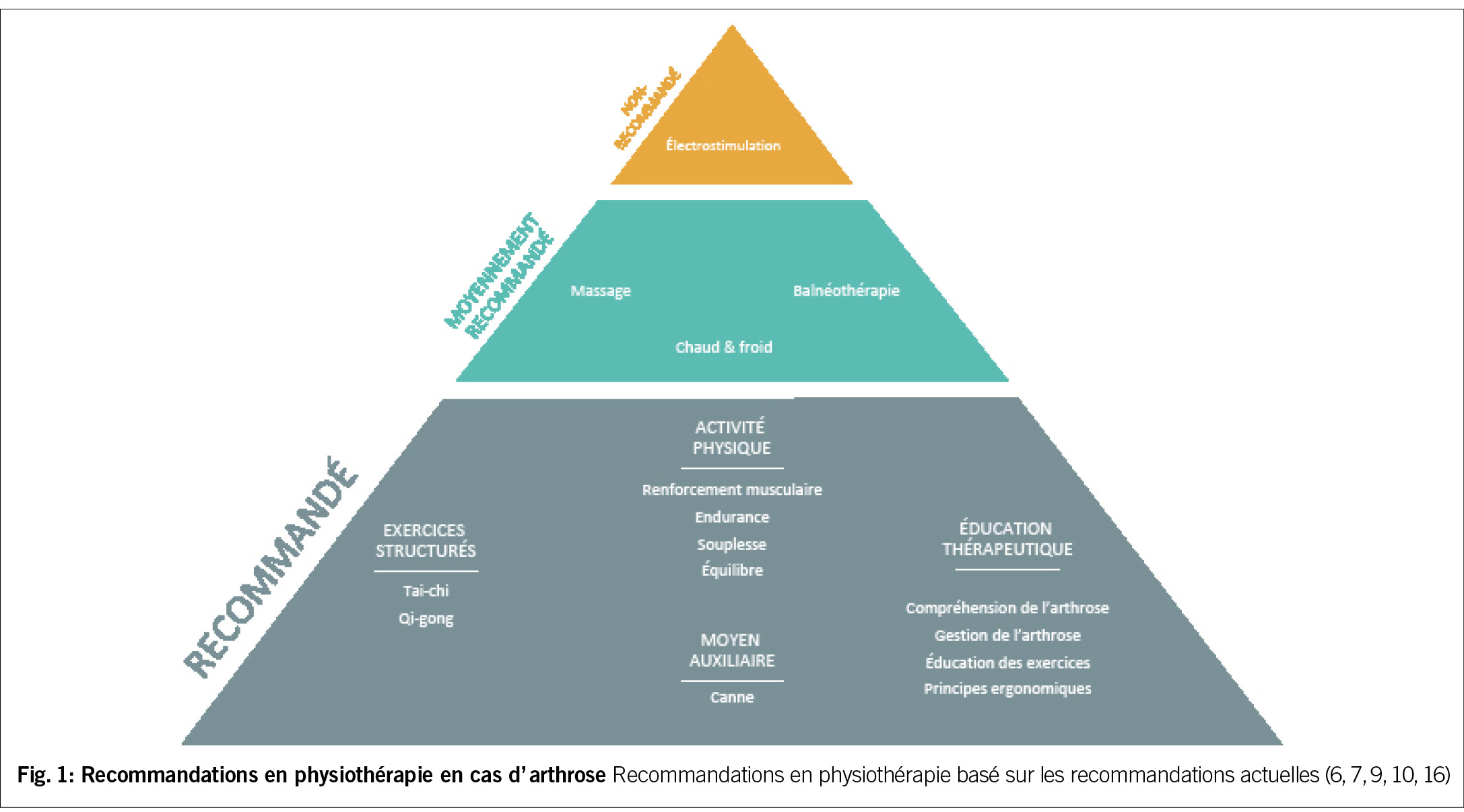
La Physiothérapie
Le physiothérapeute dans la mise en place des mesures physiques doit absolument encourager le patient à ne pas souffrir. Une évaluation initiale complète permettra au thérapeute d’ établir un programme pertinent et efficace (5). Ci-dessous, nous identifions les interventions qui sont fortement recommandées, celles qui sont considérées comme moyennement efficaces, ainsi que celles qui ne sont pas recommandées (Fig. 1). Cette classification se base sur les résultats d’ études cliniques et les avancées scientifiques dans la prise en charge de l’ arthrose.
Les massages
La faible quantité de recherches menées sur la thérapie par massage pour l’ arthrose du genou suggère qu’ elle pourrait avoir des bienfaits à court terme pour soulager la douleur du genou. Mais d’une façon générale, ce type de traitement n’ est pas recommandé (6).
Le chaud et le froid
Ces interventions incluent les sources de chaleur et de froid directes et les sources de chaleur indirectes comme la diathermie ou encore les ultrasons. La variation des méthodes de mise en œuvre de ces interventions dans les études publiées, et la courte durée des bienfaits ont conduit à une recommandation conditionnelle (6).
La balnéothérapie
La balnéothérapie a été le nom donné à la technique de baignade dans de l’ eau minérale à des fins de santé ; elle incluait également des pratiques connexes telles que les enveloppements de boue. Bien que certaines études aient signalé que ce type de balnéothérapie pouvait réduire la douleur dans l’ arthrose, Le nombre des études de bonne qualité est trop limité pour parvenir à des conclusions définitives (7).
Toutefois, l’ exercice aquatique, qui implique la réalisation d’ exercices de renforcement musculaire et d’ endurance dans une piscine, a fait état d’ avantages significatifs en termes de réduction de la douleur et d’ amélioration de la fonction (8). Il est à noter que les exercices aquatiques présentent moins d’ effets indésirables, tels que l’ inconfort, en comparaison avec le groupe d’ exercices effectués sur terre (9). Cependant les améliorations de la douleur elle-même semblent comparables entre les deux groupes (9).
Aide de marche / moyens auxiliaires
L’ utilisation de cannes est fortement recommandée pour les patients atteints d’ arthrose du genou et/ou de la hanche chez qui la maladie affecte suffisamment la démarche, la stabilité articulaire, ou provoque suffisamment de douleur pour justifier l’ utilisation d’ un dispositif d’ assistance (6). L’utilisation de genouillères et/ou de talonnettes quant à elle reste controversée (10).
L’ Activité Physique (AP)
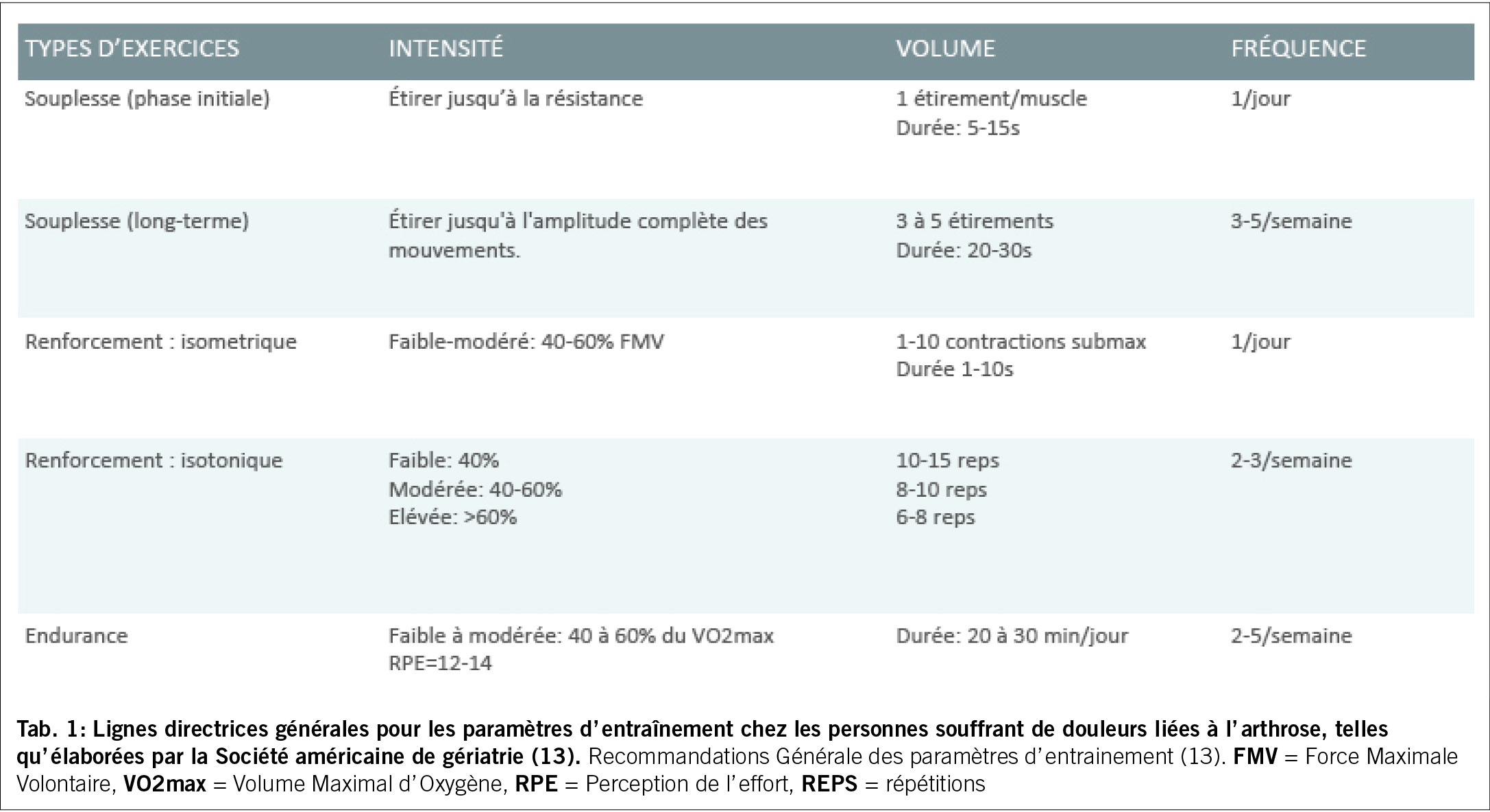
L’ exercice en général a démontré son efficacité sur la douleur (10). Il pourrait avoir différents mécanismes d’ action, outre l’ effet sur la douleur elle-même, comme l’ amélioration de la fonction en général, de la confiance, la diminution de la dépression et de l’ anxiété (11), l’ augmentation de l’ interaction sociale, l’ amélioration de la composition corporelle, ou encore l’ amélioration de la récupération du cartilage endommagé (12). Les composantes essentielles de tout programme d’ activité physique comprennent des exercices visant à améliorer la souplesse, la force et l’ endurance. Le tableau 1 présente des recommandations de base selon la Société Américaine de Gériatrie (13).
Souplesse
Bien que les étirements (stretching) ne s’ attaquent pas directement aux causes sous-jacentes de l’ arthrose, ils peuvent procurer un certain soulagement de la douleur et de l’ inconfort associés à la condition arthrosique. Des étirements doux peuvent aider à soulager la tension musculaire et favoriser la détente (10).
Renforcement musculaire
Les muscles jouent un rôle important dans la biomécanique articulaire car ils produisent le mouvement, absorbent les charges et assurent une stabilité articulaire dynamique. Cette implication dans le processus d’ adaptation et de dégénérescence articulaire lié à l’ arthrose met en évidence l’ importance de la fonction musculaire dans la prise en charge de cette pathologie (14).
Une approche ciblée est nécessaire dans l’ entraînement en force pour optimiser à la fois la protection articulaire et la fonction musculaire dans le contexte de l’ arthrose. Il a été montré que l’ entraînement en force facilite le soulagement de la douleur et renforce la capacité d’ absorption des chocs des muscles des membres inférieurs lors de la marche (11). Ces muscles, lorsqu’ ils sont utilisés en chaîne et exercés de manière statique, peuvent agir globalement comme des „amortisseurs“ pour protéger une articulation lésée. À titre d’ exemple, les triceps, les quadriceps, les ischio-jambiers, les fessiers, les abdominaux et les dorsaux contribuent à la protection de la hanche. D’ autre part ces muscles sont importants pour la fonction et devraient être ciblés de manière particulière (15).
Endurance
L’ entraînement en endurance peut favoriser le métabolisme des tissus adipeux, prévenir l’ atrophie musculaire, accélérer la récupération du cartilage endommagé et réduire la douleur (12). Le type d’ exercice en endurance peut être varié et outre le renforcement spécifique, peut inclure des activités plus globales telles que la marche, le vélo (intérêt du travail sans la contrainte du poids corporel pour le genou et la hanche) ou l’ utilisation d’ un stepper assis, en fonction de ce qui est le plus confortable et réalisable pour le patient (15). Selon plusieurs essais cliniques, l’ entraînement en force et en endurance est également recommandé pour les patients atteints d’ arthrose du genou (9).
Equilibre
L’ entraînement à l’ équilibre s’ est avéré efficace pour l’ arthrose du genou en améliorant la mobilité et en réduisant la douleur ainsi que le risque de chutes. Généralement ce travail est intégré à un programme d’ entrainement structuré ; le lien direct entre ce travail et la douleur n’ est pas encore clairement établi (6).
Exercices physiques structurés
Des programmes globaux ont montré des résultats positifs dans le soulagement des symptômes de l’ arthrose, dont la douleur. Un exemple notable est le programme GLA:D® (Good Life with osteoArthritis in Denmark), lancé au Danemark en 2013 et en Suisse en 2019, et spécialement conçu pour les personnes souffrant d’ arthrose au niveau des genoux ou des hanches (16). L’ objectif du programme GLA:D® Suisse est de mettre en œuvre les recommandations internationales de bonnes pratiques, tout en assurant un contrôle qualité rigoureux (17). Le programme combine sur plusieurs semaines des conseils, des instructions, et des exercices neuromusculaires.
D’ autre part, des séances de marche, trois fois par semaine pendant 3 mois, accompagnées d’ un suivi d’ un programme de marche à domicile sur une période de 15 mois, ont également présenté des avantages significatifs en termes de soulagement de la douleur et d’ amélioration de la fonction (9).
La participation à des activités telles que le tai-chi, comparativement à d’ autres exercices mixtes, semble offrir des améliorations plus significatives en matière de douleur liée à l’ arthrose du genou. En effet, le tai-chi démontre la capacité d’ améliorer non seulement la douleur mais aussi la raideur, le renforcement musculaire et la fonction articulaire chez les individus souffrant d’ arthrose du genou (8). Bien que le qi gong et le yoga puissent présenter des avantages similaires, des recherches plus approfondies sont nécessaires pour explorer spécifiquement les bienfaits en termes de soulagement de la douleur (8, 15).
Pour obtenir des améliorations optimales des symptômes et de la fonction, l’ utilisation d’ un programme de séances de traitement par l’ exercice, à la fois individualisées et en groupe, supervisées par un praticien spécialisé comme un physiothérapeute, suivies d’ un programme à domicile, s’ avère essentielle (15). Les programmes qui incluent aussi de l’ éducation thérapeutique, et/ou de l’ aide à la perte de poids semblent également efficaces dans la diminution de la douleur ainsi que l’ augmentation de la fonction pour l’ arthrose du genou et de la hanche (12, 18, 19).
Il n’ est pas rare que les patients ressentent une certaine gêne au niveau de l’ articulation affectée pendant l’ exercice; c’ est normal et ça ne signifie pas une détérioration de leur maladie arthrosique. Le port de chaussures appropriées, un échauffement et un arrêt progressif de l’activité adéquats, une technique d’ exercice correcte et des augmentations progressives de la dose peuvent éviter ou limiter ces symptômes (15). Des augmentations substantielles de la douleur et/ou du gonflement pendant ou après l’ exercice et qui persistent pendant plusieurs heures, peuvent suggérer que des modifications du programme d’ exercices sont nécessaires.
L’ exercice est sûr et bien toléré par la plupart des personnes atteintes d’ arthrose des membres inférieurs, même à un stade avancé, et il y a peu de contre-indications à l’ exercice résultant de l’ arthrose en soi, bien que les comorbidités doivent être prises en compte (15).
Copyright Aerzteverlag medinfo AG
PT MSc Debora Verbelen
Centre hospitalier universitaire vaudois (CHUV)
Av. de Beaumont 21 bis
1011 Lausanne
debora.verbelen@chuv.ch
PT DPT Lori Lovell-Rod
Centre hospitalier universitaire vaudois (CHUV)
Av. de Beaumont 21 bis
1011 Lausanne
michelle.lovell-rod@chuv.ch
PT PhD Laurence Vignaux
Centre hospitalier universitaire vaudois (CHUV)
Av. de Beaumont 21bis
1011 Lausanne
laurence.vignaux@chuv.ch
Les auteurs n’ ont pas déclaré de conflits d’ intérêts en rapport avec cet article.
◆ Les mesures physiques de la physiothérapie efficaces sur la douleur liée à l’arthrose se résument essentiellement aux exercices physiques.
◆ L’ approche multidimensionnelle, centrée sur des mesures physiques adaptées, permet d’ optimiser le potentiel de mouvement et de fonctionnalité tout au long de la vie. Les différentes interventions, qu’ il s’ agisse d’ exercices aquatiques, d’ entraînement en force, de marche régulière ou de programmes structurés tels que GLA:D®, démontrent des avantages significatifs en termes de soulagement de la douleur et d’ amélioration de la fonction.
◆ L’ adoption d’ un mode de vie actif et la participation régulière à des programmes d’ exercices adaptés peuvent véritablement jouer un rôle essentiel dans la gestion de la douleur et l’ amélioration de la qualité de vie des personnes touchées par l’ arthrose.
◆ A cause de l’ hétérogénéité de l’ arthrose, la thérapie par l’ exercice devrait essentiellement être individualisée et centrée sur le patient, sa maladie sa condition et ses objectifs.
◆ La littérature est plus riche pour l’ arthrose du genou, puis de la hanche, selon la prévalence plus grande ; néanmoins les douleurs d’ arthrose de la colonne vertébrale répondent bien aux exercices globaux. La littérature sur les mesures physiques et l’ arthrose des mains reste limitée.
1. Organization WH. Arthrose2023 5.1.2024 29.1.2024]. Available from: https://www.who.int/fr/news-room/fact-sheets/detail/osteoarthritis.
2. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745-59.
3. Therapy WCfP. Description of physical therapy: Policy statement2019 [cited 2019. Available from: https://world.physio/sites/default/files/2020-07/PS-2019-Description-of-physical-therapy.pdf.
4. Fu K, Robbins SR, McDougall JJ. Osteoarthritis: the genesis of pain. Rheumatology (Oxford). 2018;57(suppl_4):iv43-iv50.
5. van Baar ME, Dekker J, Oostendorp RA, Bijl D, Voorn TB, Bijlsma JW. Effectiveness of exercise in patients with osteoarthritis of hip or knee: nine months’ follow up. Ann Rheum Dis. 2001;60(12):1123-30.
6. Kolasinski SL, Neogi T, Hochberg MC, Oatis C, Guyatt G, Block J, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res (Hoboken). 2020;72(2):149-62.
7. Protano C, Fontana M, De Giorgi A, Marotta D, Cocomello N, Crucianelli S, et al. Balneotherapy for osteoarthritis: a systematic review. Rheumatol Int. 2023;43(9):1597-610.
8. Bannuru RR, Osani MC, Vaysbrot EE, Arden NK, Bennell K, Bierma-Zeinstra SMA, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1578-89.
9. Golightly YM, Allen KD, Caine DJ. A comprehensive review of the effectiveness of different exercise programs for patients with osteoarthritis. Phys Sportsmed. 2012;40(4):52-65.
10. Hurley M, Dickson K, Hallett R, Grant R, Hauari H, Walsh N, et al. Exercise interventions and patient beliefs for people with hip, knee or hip and knee osteoarthritis: a mixed methods review. Cochrane Database Syst Rev. 2018;4(4):Cd010842.
11. Tarantino D, Theysmans T, Mottola R, Verbrugghe J. High-Intensity Training for Knee Osteoarthritis: A Narrative Review. Sports (Basel). 2023;11(4).
12. Zeng CY, Zhang ZR, Tang ZM, Hua FZ. Benefits and Mechanisms of Exercise Training for Knee Osteoarthritis. Front Physiol. 2021;12:794062.
13. Exercise prescription for older adults with osteoarthritis pain: consensus practice recommendations. A supplement to the AGS Clinical Practice Guidelines on the management of chronic pain in older adults. J Am Geriatr Soc. 2001;49(6):808-23.
14. Valderrabano V, Steiger C. Treatment and Prevention of Osteoarthritis through Exercise and Sports. J Aging Res. 2010;2011:374653.
15. Bennell KL, Hinman RS. A review of the clinical evidence for exercise in osteoarthritis of the hip and knee. J Sci Med Sport. 2011;14(1):4-9.
16. Available from: www.glaid.dk.
17. [30.1.2024]. Available from: https://gladsuisse.ch/arthrose/.
18. Sinatti P, Sánchez Romero EA, Martínez-Pozas O, Villafañe JH. Effects of Patient Education on Pain and Function and Its Impact on Conservative Treatment in Elderly Patients with Pain Related to Hip and Knee Osteoarthritis: A Systematic Review. Int J Environ Res Public Health. 2022;19(10).
19. Robson EK, Hodder RK, Kamper SJ, O’ Brien KM, Williams A, Lee H, et al. Effectiveness of Weight-Loss Interventions for Reducing Pain and Disability in People With Common Musculoskeletal Disorders: A Systematic Review With Meta-Analysis. wJ Orthop Sports Phys Ther. 2020;50(6):319-33.
La disponibilité des agonistes des récepteurs du GLP-1 est actuellement limitée au niveau mondial et ne couvre pas les besoins. Comme ce groupe de médicaments joue un rôle particulier dans le traitement de l’ obésité, la question se pose actuellement de savoir quels patients devraient avoir accès en priorité à ces médicaments. Les études actuelles, SELECT et STEP-HFpEF, portant sur l’ utilisation du semaglutide chez des patients présentant des antécédents cardiovasculaires ou une insuffisance cardiaque avec fraction d’ éjection préservée, peuvent fournir des indications sur une priorité médicalement justifiée. D’ autre part, la souffrance individuelle et le désir de traitement chez les personnes souffrant d’ obésité ne correspondent pas toujours aux aspects médicaux de l’ indication de traitement. Cela rend souvent la priorisation difficile pour les médecins traitants dans le quotidien clinique.
The availability of GLP-1 receptor agonists is currently limited worldwide and does not meet demand. As this group of drugs plays a special role in the treatment of obesity, the question currently arises as to which patients should be given priority access to these drugs. The current studies, SELECT and STEP-HFpEF, on the use of semaglutide in patients with pre-existing cardiovascular disease or heart failure with preserved ejection fraction may provide indications of medically justified prioritization. On the other hand, the individual level of suffering and desire for treatment in people with obesity does not always correlate with the medical aspects of the treatment indication. This often makes prioritization difficult for the treating physicians in everyday clinical practice. Key Words: GLP-1 receptor agonists, obesity, limited availability
Nous disposons depuis quelques années de l’agoniste du GLP-1 liraglutide sous la marque Saxenda pour le traitement de l’obésité et de la surcharge pondérale en cas de comorbidités associées. En avril 2020, le médicament a été inscrit sur la liste des spécialités (LS) de l’ Office fédéral de la santé publique (OFSP) et a été largement utilisé par la suite. Comme nous l’ avons montré dans une étude récemment publiée à l’ échelle nationale, le traitement a été très efficace, mais l’ utilisation et le succès ont été restreints par les limitations de la LS (1).
Nouveau Wegovy® au lieu de Saxenda®
À l’ avenir, Saxenda® ne sera plus utilisé en Suisse pour le traitement de l’ obésité chez l’ adulte, car la société de production Novo Nordisk a actuellement mis sur le marché un nouveau médicament de la même classe de substances actives appelé Wegovy® (principe actif : sémaglutide) avec la même indication thérapeutique, qui est désormais prioritaire en raison des capacités de production limitées. Cette décision semble compréhensible pour différentes raisons et justifiée sur le plan médical. Tout d’ abord, le sémaglutide est, en ce qui concerne la réduction de poids souhaitée nettement plus efficace que le liraglutide (2).
Deuxièmement, on dispose pour la première fois de données cardiovasculaires pour le traitement de l’ obésité et de surpoids avec complications métaboliques chez des personnes sans diabète de type 2 (3, 4). Troisièmement, le sémaglutide, contrairement au liraglutide n’ est pas administré quotidiennement, mais seulement une fois par semaine par voie sous-cutanée, ce qui permet de réduire nettement la consommation de stylos injecteurs, réduisant ainsi l’impact environnemental et permettant l’utilisation plus judicieuse de stylos dont la production est limitée.
Indication et abus du semaglutide
L’ utilisation du semaglutide dans la pratique n’ est pas nouvelle, puisque la substance est disponible sous le nom commercial Ozempic® pour la forme injectable sous-cutanée et Rybelsus® pour la voie orale depuis quelques années déjà pour le traitement du diabète de type 2. Tel que rapporté dans les médias ces derniers mois, ces médicaments ont également été utilisés dans le cadre d’ applications „off label“ chez des patients souffrant de surpoids et d’ obésité sans diabète de type 2. Compte tenu des données scientifiques disponibles et du fait que le sémaglutide est déjà utilisé depuis longtemps pour le traitement du surpoids et l’ obésité, cette utilisation off label peut être considérée comme justifiée dans certains cas. Cependant, il semble qu’ il y ait eu un abus à plus grande échelle, car les indications médicales ont été insuffisamment prises en compte et que la médication a été administrée à des personnes sans surpoids ou obésité, dans le seul but d’ optimiser subjectivement la forme corporelle. Cette évolution a des conséquences négatives dramatiques pour les patients atteints de diabète de type 2, car il est parfois impossible de se procurer du semaglutide en raison de l’ indisponibilité du produit. Il est important de souligner que tant les personnes atteintes de diabète de type 2, mais aussi les personnes souffrant d’ obésité ou de surpoids avec des maladies secondaires associées sans diabète de type 2 ont une claire indication à traitement médicamenteux spécifique, étant donné que toutes les maladies mentionnées s’ accompagnent d’ une forte augmentation de la mortalité. La disponibilité restreinte des médicaments ne doit en aucun cas conduire à ce que des groupes de patients individuels soient mis en opposition les uns contre les autres, Afin de garantir un approvisionnement suffisant pour toutes les groupes de patients à l’ avenir, il est essentiel de prescrire strictement les médicaments disponibles dans les indications données.
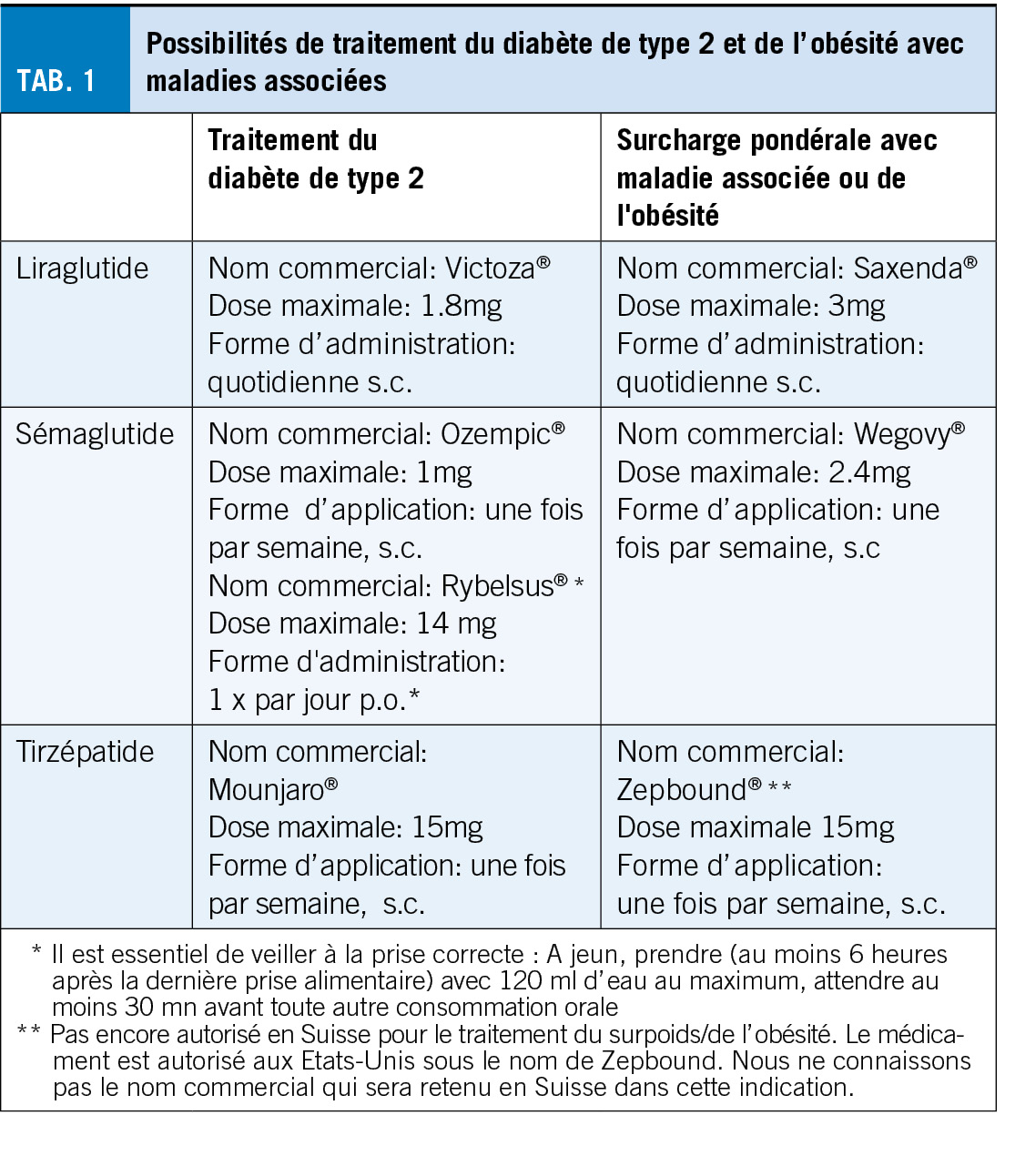
Quels médicaments pour le diabète de type 2, quels médicaments pour l’ obésité?
L’ obésité est une maladie chronique qui s’ accompagne de nombreuses séquelles et d’ une forte diminution de l’ espérance et de la qualité de vie.
Les personnes souffrant d’ obésité ont donc droit à un traitement adéquat, basé sur des preuves, comme les personnes atteintes de diabète de type 2. Ainsi, il nous semble actuellement difficilement supportable, d’ un point de vue médical et éthique, de devoir nous concentrer formellement sur le traitement du diabète de type 2 ou de l’ obésité chez certaines personnes, pour des raisons réglementaires de prise en charge des coûts, alors que les deux maladies concernent souvent la même personne. Nous souhaitons néanmoins donner ici un aperçu des substances actives autorisées, à quel dosage et sous quel nom, pour le traitement du diabète de type 2 et pour le traitement de l’ obésité ou du surpoids avec troubles associés. Le tirzépatide („Mounjaro“), un bi-agoniste qui stimule non seulement le récepteur GLP-1, mais aussi le récepteur GIP, jouera probablement un rôle important dans le traitement de toutes les maladies mentionnées dans un avenir proche, c’ est pourquoi nous l’ avons également listé dans le tableau 1. Pour plus de détails sur l’ autorisation et le remboursement, nous vous renvoyons aux publications correspondantes de Swissmedic (5) et à la liste des spécialités (6) de l’ OFSP.
Le semaglutide – toujours en pénurie et contingenté
Selon les informations fournies par le fabricant Novo Nordik, le sémaglutide sous forme d’ injection sous-cutanée ne sera toujours disponible qu’ en quantité limitée. Durant les prochains mois, les investissements massifs réalisés actuellement dans l’ extension de nouvelles capacités de production devraient certes permettre de remédier à cette situation à l’ avenir, mais cela prendra encore plusieurs années avant qu’ un approvisionnement conforme aux besoins soit assuré. Cela signifie que nous continuerons à disposer de médicaments en quantité limitée et que nous devrons établir des priorités. Concrètement, au cours des prochaines années, nous devrons décider quotidiennement quels patients seront traités en priorité avec les médicaments disponibles et quels patients devront attendre malgré le souhait de traitement et l’ indication médicale existante. Il s’ agit là d’ un défi particulier, que nous n’ avons que peu, voire pas du tout, connu en Suisse jusqu’ à présent.
Le défi de la priorisation
L’ obésité est une maladie chronique. Les interruptions du traitement médicamenteux entraînent une reprise du poids corporel (2), ce qui représente une charge émotionnelle importante pour les personnes concernées, mais a également des conséquences somatiques négatives considérables. Pour nous, la priorité absolue est donc de pouvoir poursuivre les traitements existants. C’ est pourquoi nous proposons donc aux patient traités par Saxenda jusqu’à présent ainsi qu’à ceux traités par sémaglutide en utilisation «off label» mais pour des raisons médicales justifées, de changer pour le traitement de Wegovy. Il ne faut pas oublier de mentionner que la poursuite du traitement dépend malheureusement aussi des ressources financières des personnes concernées en raison de la prise en charge des coûts limitée dans le temps jusqu’ à présent, car les traitements correspondants doivent être financés par les personnes elles-mêmes sur le long terme. Contrairement à d’ autres maladies telles que le diabète de type 2 mellitus, l’ hypertension artérielle ou le cancer, les personnes atteintes de cette maladie doivent financer elles-mêmes leur traitement. Le surpoids et l’ obésité sont également des maladies neurobiologiques non imputables à des facteurs polygéniques (7), il s’ agit d’ une situation inacceptable qui doit être corrigée d’ urgence.
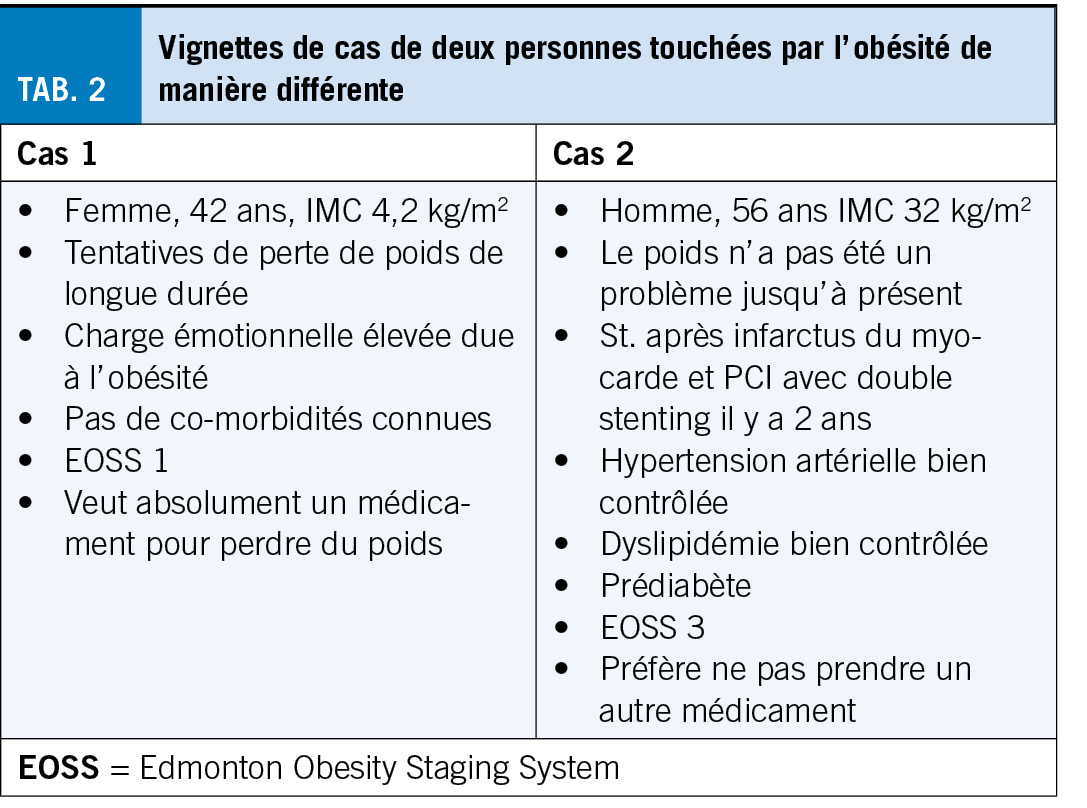
Nous pensons que la disponibilité future du sémaglutide devrait s’ améliorer progressivement, de sorte que de plus en plus de nouveaux patients pourront en bénéficier. Aujourd’ hui déjà, les centres qualifiés connaissent de longs délais d’ attente pour les personnes souhaitant être traitées sur la base d’ une indication médicale claire. La question des priorités se pose avec acuité, au plus tard en face de ces longs d’elais d’attente. Pour illustrer ce dilemme de manière tangible dans le quotidien clinique, nous décrivons deux patients rencontrés dans la pratique quotidienne (encadré 1). Qui traiteriez-vous en premier? La patiente qui souffre énormément et qui souhaite absolument un traitement? Ou plutôt le patient qui ne souhaite pas vraiment de traitement et qu’il faudrait probablement encourager à débuter un traitement?
Études cardiovasculaires
Pour prendre de bonnes décisions cliniques, il est important, même si ce n’ est pas toujours suffisant, de connaître les données scientifiques disponibles. L’ étude SELECT récemment publiée (3) est particulièrement pertinente dans le contexte de la priorisation de l’ utilisation du sémaglutide. Cette étude a porté sur des personnes ayant un IMC d’ au moins 27 kg/m2 et souffrant d’ une maladie cardiovasculaire (infarctus du myocarde survenu, accident vasculaire cérébral ou maladie artérielle périphérique). Au total, 17604 personnes ont été randomisées 1:1 pour recevoir soit un placebo, soit 2,4 mg de sémaglutide, 1 fois par semaine, s.c. Le critère d’ évaluation primaire combiné était le décès d’ origine cardiovasculaire, l’ infarctus du myocarde non fatal ou l’ accident vasculaire cérébral non fatal (MACE à 3 pts). L’ étude s’ est terminée après une durée moyenne de traitement de près de 40 mois, après la survenue d’ un nombre prédéfini (1’ 225) d’ événements du critère d’ évaluation primaire. Le résultat a montré que le traitement par le sémagutide a permis de réduire de 20% la survenue du critère d’ évaluation primaire par rapport au traitement par placebo (placebo vs. sémaglutide : 8,0% vs 6,55, hazard ratio 0,80 ; 95% intervalle de confidence 0. 72- 0.90; P<0.001). La réduction absolue du risque était donc de 1.5%, ce qui signifie qu’ environ 67 personnes présentant les caractéristiques cliniques correspondantes devraient être traitées par le sémaglutide pendant 40 mois pour éviter l’ un des critères d’ évaluation primaires.
Une autre étude semble également pertinente dans le cadre de la priorisation. Il s’ agit de l’ étude STEP-HFpEF, qui a inclus des personnes présentant un IMC d’ au moins 30kg/m2 et une insuffisance cardiaque avec fraction d’ éjection préservée (FE >45%, NYHA II-IV) (4). 529 personnes ont été randomisées 1:1 pour recevoir soit 2,4mg de sémaglutide par semaine, soit un placebo, et ont été traitées pendant 52 mois. Outre les effets sur le poids corporel, l’ amélioration de la symptomatologie et des fonctions physiques ont été définies comme critère d’ évaluation primaire. Les résultats ont montré qu’ après 20 semaines de traitement par le sémaglutide, l’ amélioration des symptômes de l’ insuffisance cardiaque était déjà nettement plus importante que sous placebo et que la différence entre les groupes de traitement augmentait avec la durée du traitement. Lors d’ un test de marche de 6 minutes, la distance de marche s’ est allongée de 21,5 mètres sous sémaglutide, alors qu’ elle ne s’ est améliorée que de 1,2 mètre sous placebo (différence de 20,3 mètres ; intervalle de confiance à 95% : 8,6 -32,1 ; p<0,001).
Qui devrait maintenant être traité en priorité?
Revenons à nos deux cas: il n’ est pas facile de décider qui doit être traité en priorité par le sémaglutide. La plupart d’ entre nous seront probablement enclins à traiter en premier la patiente (cas 1) qui souffre beaucoup et qui a une forte envie de traitement. Cependant, cette patiente a une indication claire pour une chirurgie bariatrique, pour laquelle elle a été jugée apte en raison de son obésité marquée et de ses longues années de tentative de perte de poids (8, 9). Dans ce contexte, il convient de rappeler une fois de plus les effets impressionnants de la chirurgie bariatrique sur la prolongation de la vie (10). Basé sur les dates publiées, il est clair que le patient (cas 2) doit être traité prioritairement par le sémaglutide.
Du point de vue de l’ économie de la santé, cela pourrait avoir du sens, si l’ on considère que chez le patient 2 il y a une chance de prévenir un autre accident cardiovasculaire grave dans les années à venir, et donc d’ économiser les coûts du traitement correspondants. Dans une telle considération médicale, plutôt théorique, on perd toutefois de vue la perspective des patients, qui devrait également être prise en compte dans la prise des décisions. En fin de compte, il n’ y aura pas de réponse de principe à la question de la priorisation. Il n’ y a pas de bonne ou de mauvaise réponse, car chaque cas doit être examiné individuellement. Les directives réglementaires, qui sont actuellement en cours d’ élaboration par les sociétés savantes suisses concernées peuvent aider les différents décideurs dans cette situation et offrir un soutien pratique et un certain soulagement en ce qui concerne la responsabilité de la prise de décision.
À quoi ressemblera l’ avenir?
On peut s’ attendre à ce que les pénuries et les retards de livraison soient surmontés. En outre, il y aura toute une série de nouvelles préparations avec des effets similaires, ce qui élargira le choix et la disponibilité des médicaments pour le traitement pharmacologique de l’ obésité, et améliorera encore la situation. En plus du médicament déjà mentionné, le tirazépatide, des substances basées également sur un effet GLP-1 et parfois d’ autres effets supplémentaires, sont actuellement en cours dans des programmes d’ études de phase 2 et de phase 3 (11, 12). Même si les résultats de ces études doivent être attendues, on peut déjà affirmer le grand espoir de voir s’ élargir la palette des options thérapeutiques pour le traitement pharmacologique de l’ obésité à l’ avenir. Il convient de mentionner que de nouvelles substances à base de peptides, aussi des „petites molécules“ qui peuvent être prises par voie orale sont à l’ étude et pourraient ainsi être utilisées à moindre coût (13). Si l’ on considère le grand nombre de personnes qui pourraient bénéficier d’ un tel traitement, cela souligne l’ importance de l’ aspect des coûts, car il s’ agit en fin de compte de la possibilité de financer un traitement de longue durée pour une grande partie de la population. À cet égard, la charge socio-économique élevée que représentent pour la société les nombreuses maladies consécutives à l’ obésité extrêmement coûteuses, qui peuvent être évitées grâce aux nouveaux médicaments doivent être prises en compte. La dépendance d’ un traitement médicamenteux efficace de l’ obésité des possibilités financières aux ressources individuelles des personnes concernées est inacceptable, tant du point de vue médical que d’ un point de vue social, car elle ne correspond pas à notre exigence d’ une société socialement équitable. Même s’ il faut attendre les résultats de ces études, on peut déjà espérer que la palette des options thérapeutiques pour le traitement de l’ obésité s’ élargira.
Conclusion
La disponibilité limitée de médicaments contre l’ obésité en général et le sémaglutide en particulier pose actuellement de nouveaux défis importants qui nécessitent une priorisation inhabituelle. Même si le manque de disponibilité sera résolu dans quelques années, les ressources financières limitées du système de santé laissent craindre que dans le futur, des priorités soient fixées pour certains traitements. Dans ce contexte, les expériences dans le domaine de l’ obésité que nous sommes en train d’ acquérir seront aussi précieuses pour les processus décisionnels médicaux futures d’ économie de la santé.
Cet article est une traduction de «der informierte arzt – die informierte ärztin» 02_2024
Copyright Aerzteverlag medinfo AG
Pr Dr Bernd Schultes
Centre du métabolisme de Saint-Gall
friendlyDocs AG
Lerchentalstrasse 21
9016 St. Gallen
stoffwechselzentrum@friendlydocs.ch
Pr Dr Gottfried Rudofsky
Cabinet d’ endocrinologie, de diabète et d’obésité
Baslerstrasse 30
4600 Olten
endokrinologie-olten@hin.ch
Pre Katharina Timper
Clinique d’endocrinologie, de diabétologie et
de métabolisme Hôpital universitaire de Bâle
Petersgraben 4
4031 Bâle
Département de biomédecine, Université de Bâle
Bernd Schultes : Les honoraires de conférence et de conseil de Novo Nordisk et Eli Lilly, ainsi qu’ un soutien financier à la recherche par Novo Nordisk. Gottfried Rudofsky :
honoraires de conférenciers et honoraires de conseil de Novo Nordisk et Eli Lilly. Katharina Timper: honoraires de conférence et honoraires de conseil de Novo Nordisk, Eli Lilly, et Boehringer-Ingelheim, ainsi qu’ un soutien financier à la recherche de la part de Novartis et Novo Nordisc.
Les troubles tels que « fatigue », « somnolence », besoin de sommeil prolongé avec réveil difficile (hypersomnie) ou « épuisement » avec durée de récupération prolongé doivent être définis le mieux possible par des questions ciblées en raison des conséquences thérapeutiques. En cas de fatigue ou de somnolence diurne, il convient d’ envisager à temps une narcolepsie, en plus des causes fréquentes telles que le manque de sommeil, l’ apnée du sommeil et la dépression. En règle générale, une vidéo-polysomnographie est indispensable pour exclure les troubles respiratoires ou moteurs liés au sommeil. En cas de suspicion de narcolepsie ou d’ hypersomnie, elle doit être complétée par l’ actigraphie et un test de latence au sommeil (MSLT). Le médecin traitant doit informer chaque patient souffrant de somnolence diurne, dès la première consultation, de sa grande responsabilité au volant et, en cas de doute, l’ adresser à un centre du sommeil pour un test de maintien de l’ éveil (TME).
Complaints such as «tiredness», «sleepiness», prolonged need for sleep with difficult awakening (hypersomnia) or «exhaustion» with prolonged recovery time must be defined as precisely as possible with targeted questions because of the therapeutic consequences. In the case of any tiredness or sleepiness, narcolepsy should be considered at an early stage in addition to the common causes such as sleep deficiency, sleep apnea and depression. As a rule, a video-polysomnography is necessary to exclude sleep-related breathing or movement disorders. If narcolepsy or hypersomnia is suspected, actigraphy and multiple sleep latency test (MSLT) should be added. The attending physician should inform every patient with daytime sleepiness already at the first consultation about his great responsibility at the wheel and refer the patient in case of doubt to a sleep center for a maintenance of wakefulness test (MWT). Key Words: Hypersomnolence centrale, somnolence diurne, hypersomnie, narcolepsie, fatigue, syndrome de fatigue chronique
La « somnolence diurne », l’ « hypersomnie », la « fatigue » ou l’ « épuisement » (fatigue) sont des symptômes fréquents dans le cabinet de chaque médecin, qui nécessitent un diagnostic aussi précis que possible avant qu’ une thérapie et des conseils ciblés ne soient possibles (1, 2, 3). Lors de l’ anamnèse, il convient tout d’ abord de clarifier autant que possible ce que le patient entend par ses troubles, même s’ il faut être conscient que plusieurs troubles peuvent être présents simultanément.
Terminologie
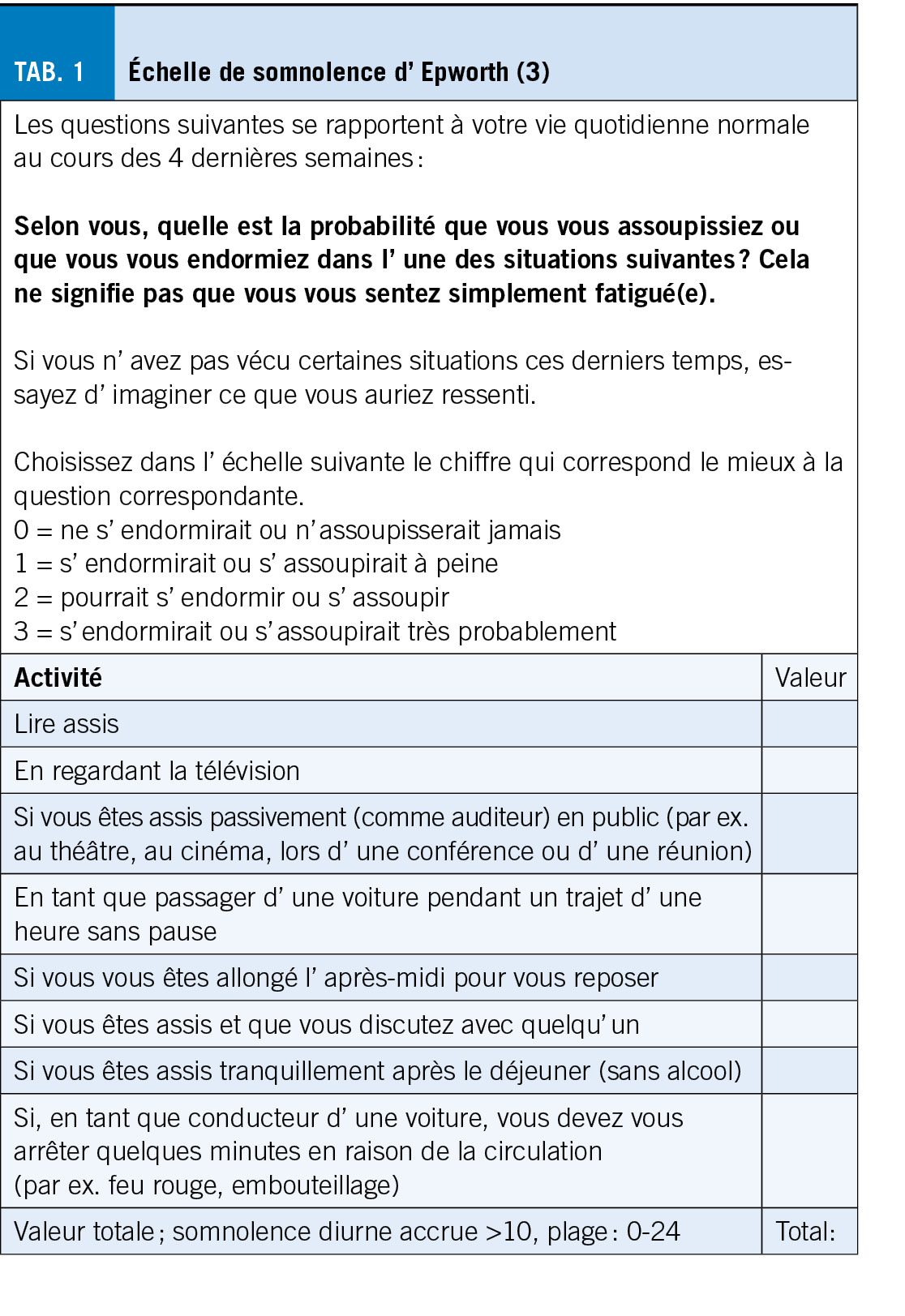
Le terme « somnolence diurne » est utilisé pour désigner l’ augmentation de la pression de sommeil pendant la journée avec des endormissements fréquents dans des situations passives ou même actives. Contrairement à la fatigue, la somnolence s’ améliore lors d’ activités physiques et généralement aussi après une power-nap. Une somnolence diurne se traduit par un score élevé (>10/24 points) au questionnaire d’ Epworth (tab. 1) et peut être objectivée par une latence moyenne d’ endormissement raccourcie (< 10 minutes) au test de latence au sommeil (MSLT).
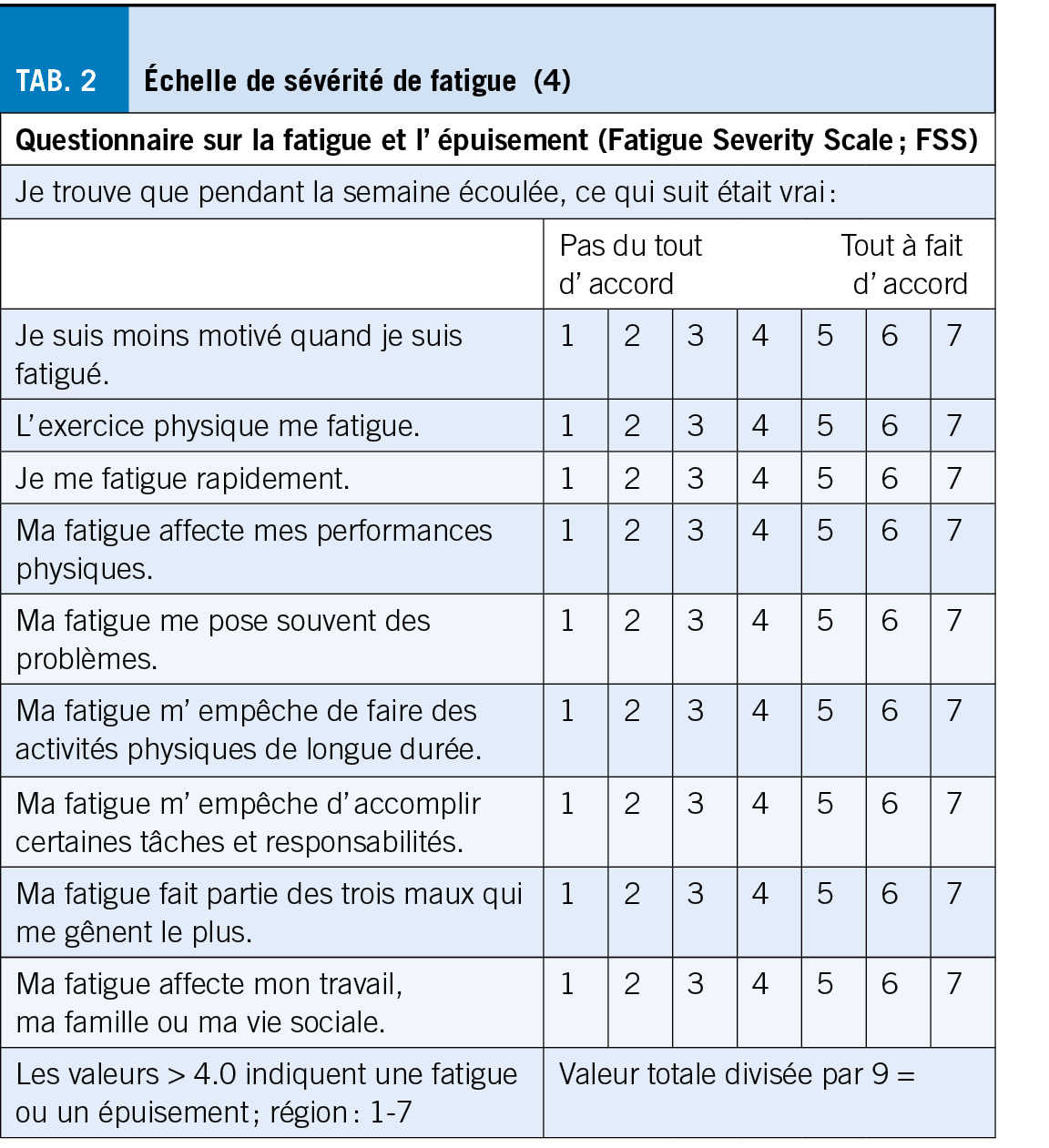
Le terme « hypersomnie » désigne un besoin de sommeil de >11 heures par 24 heures, généralement associé à un réveil difficile parce que le réveil n’ est pas entendu. La meilleure méthode pour quantifier l’ hypersomnie est la polysomnographie (PSG) « ad libitum », au cours de laquelle le patient peut faire la grasse matinée. Le terme « fatigue » est utilisé pour désigner la sensation d’ un manque d’ énergie prononcé, qui s’ accroît encore en cas d’ activité mentale ou physique. Le score de fatigue (4) (tab. 2) est nettement augmenté, le score d’ Epworth peut également être augmenté ou normal. La latence à l’ endormissement lors du test MSLT est cependant généralement normale (>10 minutes). Le lever matinal est également souvent retardé, non pas parce que le réveil n’ est pas entendu, mais parce que l’ énergie pour se lever manque après le réveil (= clinophilie). Le terme « épuisement (fatigue) » décrit la baisse de performance au cours d’ un effort mental ou physique, généralement suivie d’ un temps de récupération fortement prolongé (> 1 heure à une journée entière) avec un fort désir de repos mais pas forcément de sommeil.
Les causes
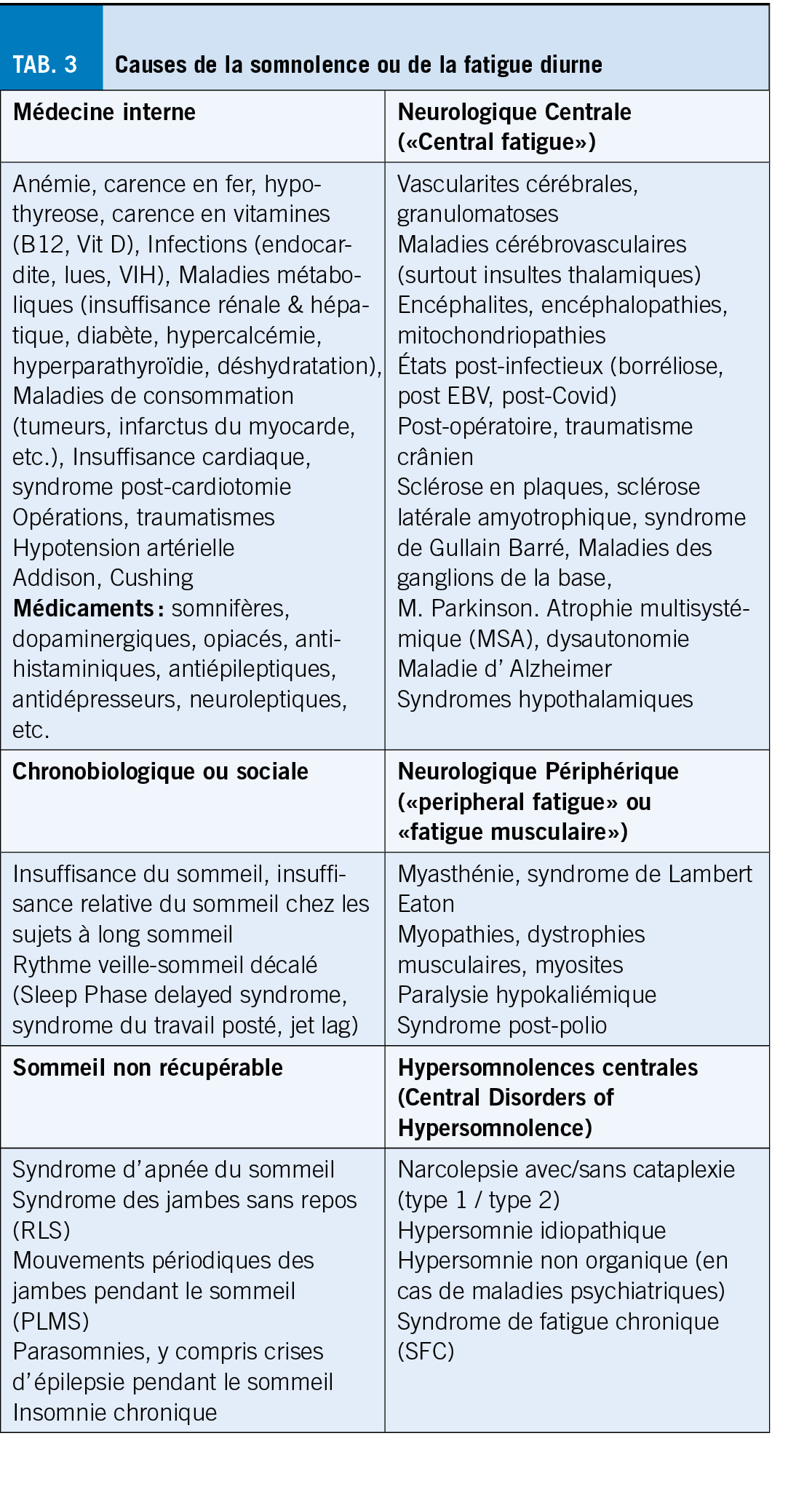
En plus de l’ anamnèse détaillée, y compris l’ évolution longitudinale et les éventuels liens avec des maladies somatiques ou psychiatriques, et d’ un examen clinique, le médecin de famille effectuera également quelques examens de laboratoire pour exclure des causes internes (tab. 3). La mise en évidence en laboratoire d’ une hypothyroïdie, d’ une anémie ou d’ une carence en fer ne devrait toutefois que rarement constituer la seule explication d’ une fatigue chronique ou d’ une somnolence.
La fréquente insuffisance de sommeil d’ origine sociale ou une hygiène du sommeil déficiente avec des heures de coucher et de lever variables et un rythme veille-sommeil décalé doivent être exclus dans une période de test de quelques semaines avec un rythme régulier et une durée de sommeil adaptée individuellement. Une insuffisance de sommeil d’ origine sociale d’ une heure par nuit par rapport au besoin de sommeil individuel peut déjà entraîner une somnolence/fatigue diurne. Le décalage du rythme veille-sommeil, qui apparaît surtout à l’ adolescence, se caractérise par l’ apparition simultanée d’ une insomnie d’ endormissement et d’ un réveil difficile, qui disparaît pendant les vacances lorsque le rythme est « libre ».
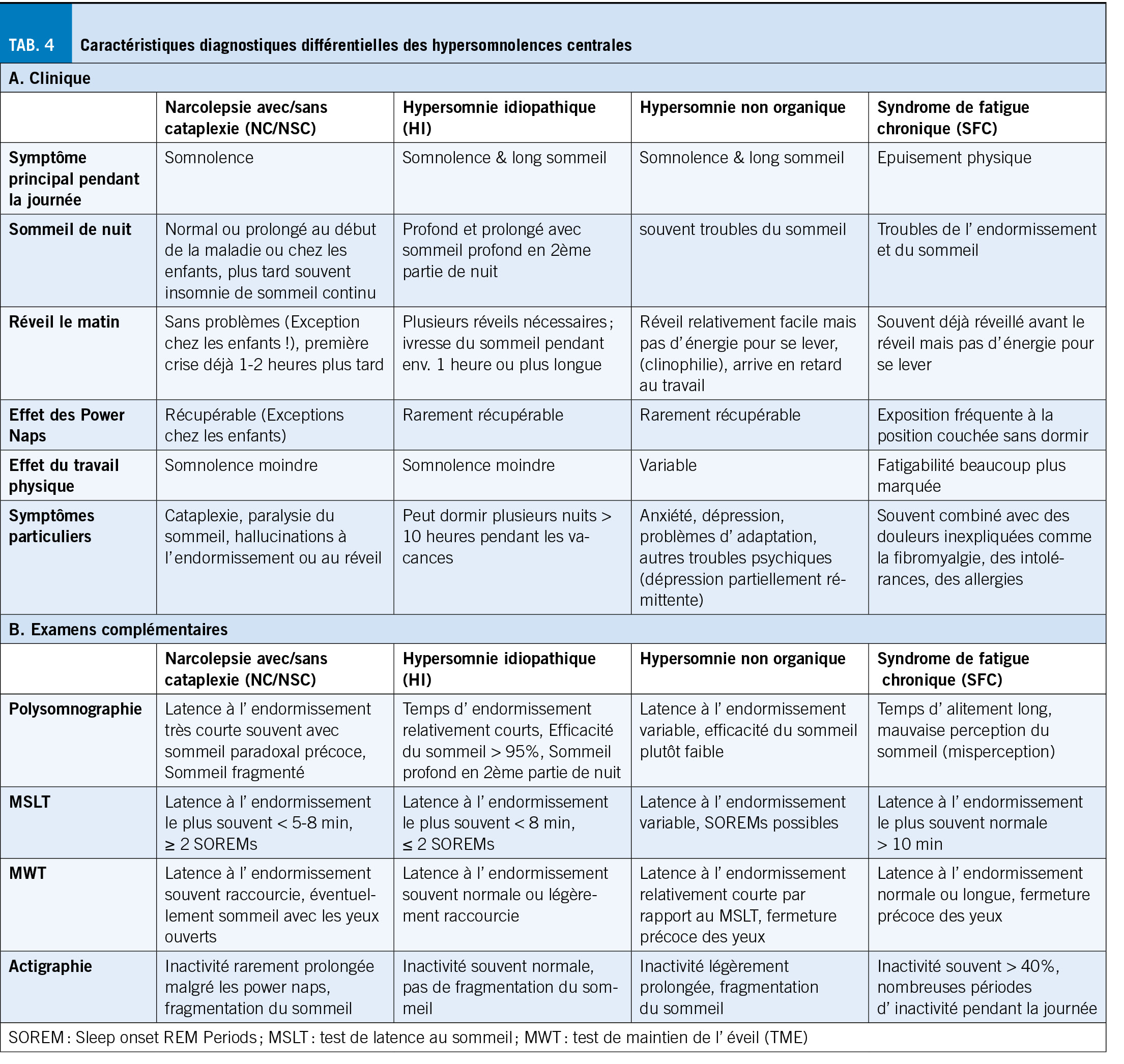
L’ étape suivante consiste à déterminer, au moyen d’ une vidéo-polysomnographie (PSG), les causes les plus fréquentes du sommeil non récupérable, telles que les troubles respiratoires et moteurs liés au sommeil et diverses parasomnies, y compris les crises d’ épilepsie pendant le sommeil (1). Dans le cas du syndrome d’ apnées obstructives du sommeil, la somnolence diurne ou la fatigue sont bien connues. En revanche, la relation de cause à effet entre un indice élevé de mouvements périodiques des jambes pendant le sommeil (PLMS) et une fatigue ne devrait pas être présumée d’ emblée, tant qu’ un traitement probatoire des PLMS n’ a pas permis d’ améliorer la fatigue. Une fois que le sommeil non récupérable a été exclu, il reste un petit groupe d’ « hypersomnolences centrales », dont font partie, outre la narcolepsie avec ou sans cataplexie, l’ hypersomnie idiopathique (HI) et l’ hypersomnie non organique. En raison des séquences thérapeutiques, ces causes doivent être distinguées et différenciées du syndrome de fatigue chronique (SFC) (7). Le diagnostic est posé sur la base des symptômes cliniques typiques (tab. 4A) et des résultats des examens complémentaires de médecine du sommeil (tab. 4B).
On distingue la narcolepsie avec cataplexie (NC ; type 1) de la narcolepsie sans cataplexie (NSC; narcolepsie monosymptomatique ; type 2) (1, 2).
Il s’ agit d’ un trouble potentiellement invalidant de la « structure du sommeil et de l’ éveil », caractérisé par la pentade 1. attaques de sommeil, 2. pertes de tonus affectif (cataplexie ; type 1 uniquement), 3. hallucinations hypnagogiques, 4. paralysies du sommeil et 5. troubles de sommeil nocturne, y compris des rêves perturbants. La maladie débute souvent entre 15 et 25 ans, pendant l’ apprentissage ou l’ école, mais plus rarement bien plus tard. La plupart du temps, la somnolence diurne extrême apparaît en premier et les cataplexies souvent au cours des mois suivants, mais rarement des années plus tard, voire jamais dans le cas du type 2. Des hallucinations hypnagogiques ou des paralysies du sommeil sont décrites par environ 60 % des patients, mais ne sont pas spécifiques pour la narcolepsie.
La somnolence diurne prononcée, souvent avec un score d’ Epworth > 15 points et/ou sous forme de crises d’ endormissement irrésistibles avec des actions automatiques dans le demi-sommeil, est pratiquement toujours la plainte principale. Les adultes font généralement état d’ un réveil sans problème le matin, voire d’ une insomnie de la nuit et d’ un sommeil diurne récupérable. Les enfants et les adolescents indiquent plus souvent un besoin de sommeil prolongé par 24 heures avec un réveil difficile et des siestes non récupérables.
Le type 1 se caractérise par des crises de faiblesse (= cataplexie) de la musculature de la nuque, des paupières, de la mâchoire inférieure ou une dysarthrie, déclenchées après les premières secondes de l’ émotion. La faiblesse dans les genoux est fréquente, mais moins spécifique de la narcolepsie. Pour un diagnostic clair, surtout pour la recherche, mais aussi en l’ absence de cataplexie classique, un taux d’ hypocrétine fortement réduit dans le liquide céphalorachidien (LCR) est diagnostique en cas d’ une NC.
La cause de la narcolepsie est supposée être une réaction auto-immune avec une production d’ hypocrétine largement absente dans l’ hypothalamus latéral, ce qui se produit chez les personnes génétiquement prédisposées avec un HLA DQB1*0602 positif, spontanément ou après certaines influences exogènes comme par exemple une infection streptococcique ou virale et très rarement après une vaccination (6).
L’ hypersomnie idiopathique se caractérise par une augmentation du besoin de sommeil de plus de 2 heures par rapport au passé ou à une valeur > 11 heures par jour. Typiquement, ces patients présentent un réveil difficile et des siestes diurnes non récupérables, ce qui doit également être pris en compte dans la thérapie comportementale, car une prolongation supplémentaire de la durée du sommeil n’ entraîne pas d’ amélioration de la vigilance diurne.
L’ hypersomnie non organique s’ observe souvent dans le cadre d’ une dépression partiellement rémittente et peut être suspectée par le début et l’ évolution parallèle des symptômes affectifs
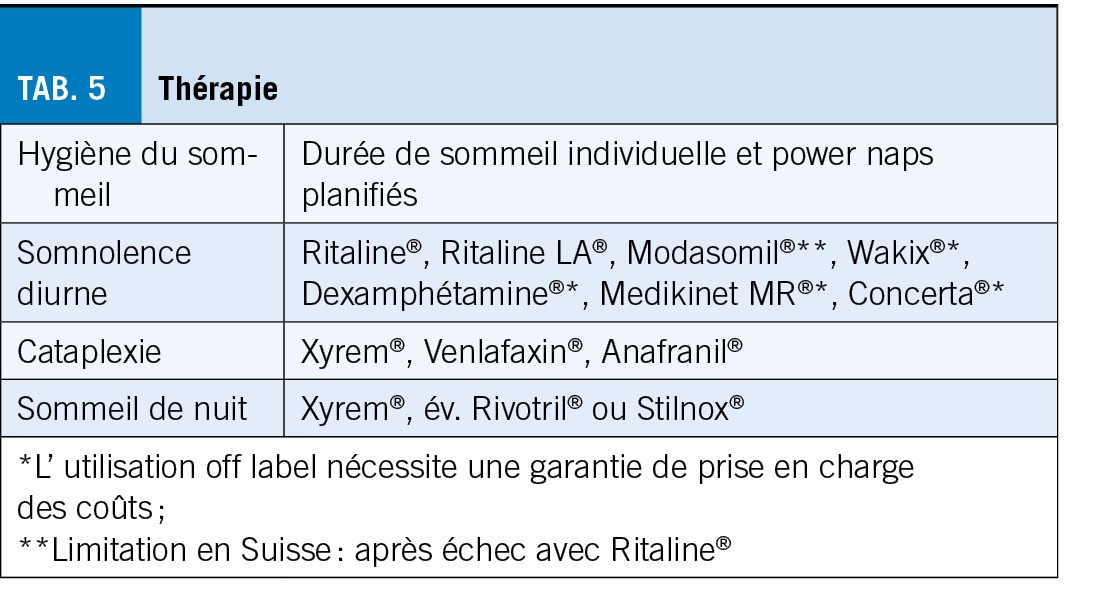
Thérapie et conseil
Le traitement est axé sur les symptômes et se compose de mesures non médicamenteuses et médicamenteuses (tab. 5), dans le but de réussir l’ école ou l’ apprentissage et de permettre l’ exercice de la profession apprise. Pour lutter contre la somnolence diurne, on associe des pauses de sommeil fixes pendant la journée à des stimulants comme le Modasomil®, la Ritaline® ou, « off label », le Wakix®, le Sunosi® ou les amphétamines. Pour le traitement des cataplexies, Xyrem® est aujourd’ hui considéré comme un médicament de premier choix, qui a en même temps un effet positif sur le sommeil nocturne souvent fragmenté et qui, de manière intéressante, peut également atténuer les difficultés de réveil le matin en cas d’ hypersomnie idiopathique (8). En cas de causes non organiques et surtout en cas de syndrome de fatigue chronique, le traitement de premier choix consiste en un programme d’ entraînement progressif dans le cadre d’ une thérapie comportementale, soutenu par des antidépresseurs activateurs (Wellbutrin®, Venlafaxine®).
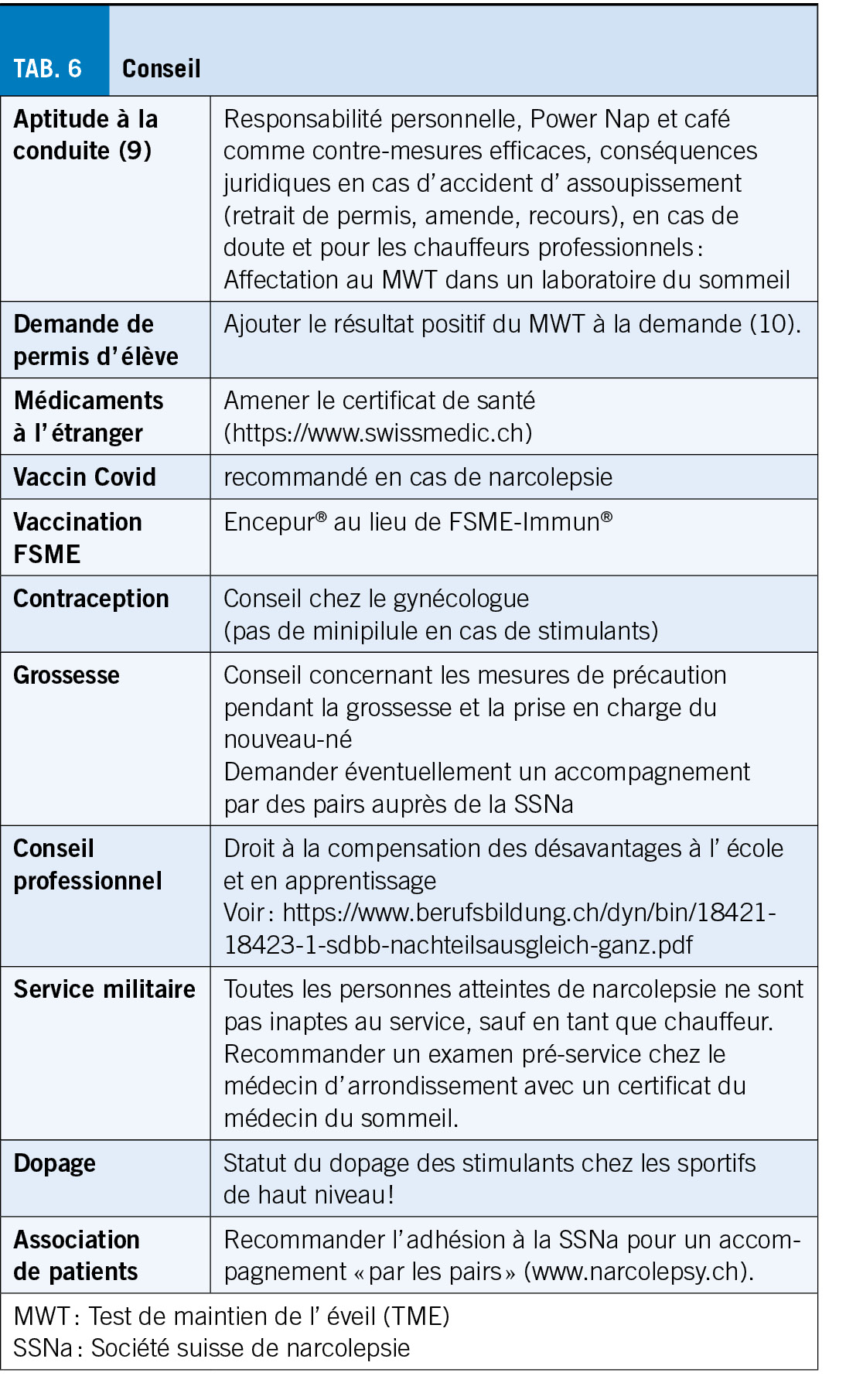
Le conseil porte sur le choix d’ une profession, les possibilités de compensation des désavantages à l’ école et en apprentissage, le planning familial, l’ aptitude à la conduite et, selon les activités, sur d’ autres domaines de la vie, une étroite collaboration entre le patient, le médecin de famille, le spécialiste du sommeil et, selon la situation, les employeurs et les psychologues étant un grand avantage (tab. 6). L’ association de patients (www.narcolepsy.ch) offre la possibilité d’ un accompagnement par d’ autres personnes concernées qui ont déjà fait l’ expérience de stratégies d’ adaptation (système de pairs).
Cet article est une traduction de « der informierte arzt – die informierte ärztin» 10_2022
Copyright Aerzteverlag medinfo AG
Pr Johannes Mathis
Consultation de médecine du sommeil,
Neurozentrum Bern
Schänzlistrasse 45
3013 Berne
johannes.mathis@hin.ch
L’ auteur n’ a pas déclaré de conflits d’ intérêts en rapport avec cet article.
1. Mathis J. and Hatzinger M. Praktische Diagnostik bei Müdigkeit/Schläfrigkeit. Schweizer Archiv für Neurologie und Psychiatrie 2011; 162:300-9
2. International Classification of Sleep Disorders (ICSD), 3. Aufl. American Academy
of Sleep Medicine: 2014
3. Stadje R, Dornieden K, Baum E, et.al. The differentil diagnois of tiredness:
a systematic review. BMC Family Practice 2016; 17: 1-11
4. Bloch KE, Schoch OD, Zhang JN, Russi EW. German version of the Epworth Sleepiness Scale. Respiration 1999; 66(5):440-447.
5. Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol. 1989;46:1121–3.
6. J. Mathis, S. Strozzi. Narkolepsie, eine Folge der H1N1-Grippeimpfung? Schweiz. Med. Forum 2012; 12: 8-10
7. Mathis J. Narkolepsie und andere «Zentrale Hypersomnolenzen». Praxis 107: 1161-1167 (2018)
8. Leu-Semenescu, Smaranda; Louis, Pauline; Arnulf, Isabelle (2016): Benefits and risk of sodium oxybate in idiopathic hypersomnia versus narcolepsy type 1: a chart review. Sleep Medicine 17, S. 38–44. DOI: 10.1016/j.sleep.2015.10.005.
9. Mathis J, Seeger R, Ewert U. Excessive daytime sleepiness, crashes and driving capability. Schweizer Archiv für Neurologie und Psychiatrie 2003; 154:329-338.
10. Mathis J, Kohler M, Hemmeter U-M, Seeger R. Fahreignung bei Tagesschläfrigkeit: Empfehlungen für Ärzte und akkreditierte Zentren für Schlafmedizin. Swiss Med Forum 2017; 17: 442-447 oder www.swiss-sleep.ch/driving