Hospital at Home als international anerkanntes Versorgungskonzept
Unter dem Begriff Hospital at Home (HaH) versteht man eine Versorgungsform, bei der somatisch akut erkrankten, hospitalisationspflichtigen Patient/-innen eine spitaläquivalente Behandlung zu Hause statt im Spital ermöglicht wird. HaH ist nicht für alle spitalbedürftigen Patienten geeignet, aber für eine ausgewählte Zielgruppe, bei der eine sichere, medizinisch-pflegerische Versorgung und Behandlung im häuslichen Umfeld möglich ist.
Mit dem HaH-Ansatz soll die Gesundheitsversorgung wieder näher zu den Menschen gebracht werden und sowohl der Genesungsfortschritt (u. a. besserer Schlaf durch gewohnte Umgebung und Versorgung durch Angehörige) als auch die Sicherheit von Patient/-innen (u. a. Reduktion des Infektionsrisikos, Vermeidung von Delir, geringerer Schlafmittel- und Sedativaverbrauch, weniger Stürze und Frakturen) erhöht und der Ressourcenverbrauch im Gesundheitswesen reduziert werden (1, 2). Internationale Studien zeigen zudem, dass die Autonomie der Patient/-innen zu Hause gestärkt wird und dadurch deren Unabhängigkeit leichter aufrechterhalten oder wiederhergestellt werden kann (3, 4), was nachhaltig zur Gesundheitsförderung beiträgt.
Darüber hinaus fördern die Patientenzentrierung und die intra- und interprofessionelle Zusammenarbeit in der neuen Versorgungsform eine Steigerung der Berufszufriedenheit oder -attraktivität (5, 6), wodurch man sich eine längere Berufsverweildauer des medizinischen und pflegerischen Personals erhofft.
International, insbesondere in den USA, Israel, Spanien und UK, ist HaH ein fixer Bestandteil des Gesundheitswesens (7). Eine Cochrane-Review, basierend auf 20 randomisierten Studien zu HaH, wies eine hohe Sicherheit der Patient/-innen, niedrigere Komplikationsraten als im klassisch stationären Setting, geringere Behandlungskosten und eine hohe Zufriedenheit der Patient/-innen aus (8). In der Schweiz stellt HaH ein neues Versorgungsmodell im Gesundheitswesen dar, welches in einer zunehmenden Anzahl von Projekten angeboten und erprobt wird (9).
Die Klinik Arlesheim gehört zu den Pionieren von HaH in der Schweiz, wo die neue Versorgungsform seit Januar 2023 in einem Team von Ärzt/-innen und Pflegefachpersonen implementiert wurde (10). Nach einer Machbarkeitsprüfung und Entwicklungsphase in den Jahren 2020 bis 2022 wurden von Januar bis Juni 2023 die ersten Patient/-innen im Rahmen von HaH behandelt. Seit Juni 2023 wird ein relatives feststehendes Konzept im Rahmen einer Pilot- und Evaluationsphase angeboten, welches durch den Kanton Basel-Landschaft unterstützt wird. Seit Beginn im Juni 2023 bis Ende Februar 2025 wurden ca. 350 Patient/-innen spitaläquivalent zu Hause behandelt.
Nachfolgend soll am Beispiel der Klinik Arlesheim ein Einblick gegeben werden, wie ein solches HaH-Programm praktisch funktioniert und welche Wirkungen und Möglichkeiten die neue Versorgungsform mit sich bringt. Weiterhin werden erste Ergebnisse hinsichtlich der Versorgungssicherheit, Behandlungsqualität und Zufriedenheit dargestellt.
Das Pilotprojekt an der Klinik Arlesheim
Motivation und Zielsetzung
Für das Team von Hospital at Home sind die medizinische Versorgungs- und Behandlungsqualität und die Sicherheit der Patient/-innen höchste Priorität. Das Angebot einer HaH-Behandlung ist freiwillig, und die Patient/-innen können selbst entscheiden, ob sie das Angebot annehmen oder wie sie herkömmlich im klassischen stationären Setting behandelt werden möchten. An- und Zugehörige werden im Rahmen der Behandlung miteinbezogen, beraten und angeleitet.
Parallel zur Versorgung der Patient/-innen entwickelt das Team von Hospital at Home gemeinsam mit dem Verein hospitales ein mögliches, helvetisiertes Konzept «Hospital at Home» weiter und widmet sich der Team- und Organisationsentwicklung mit modernen Arbeits- und Organisationsformen. Dabei setzt das HaH-Team in Arlesheim auf einen hohen Grad an Selbstwirksamkeit eines jeden Mitarbeitenden und arbeitet mit flachen Hierarchien und einer besonderen Meetingkultur, die eine Mitbestimmung und -gestaltung des gesamten Teams ermöglichen.
Praktisches Vorgehen
Team Klinik Arlesheim
Das HaH-Team besteht aus festangestellten, erfahrenen internistischen Fachärzt/-innen und Assistenzärzt/-innen und aus diplomierten Pflegefachkräften. Alle Teammitglieder sind mit der Versorgung internistischer Patient/-innen im stationären Setting vertraut. Eine enge Zusammenarbeit mit Therapeut/-innen, Spitex (spitalexterne Hilfe und Pflege), Hausärzt/-innen, Radiologieinstituten und Fachärzt/-innen (Konsile) besteht, und diese können situativ zugezogen werden.
Zuweisung und Patientenaufnahme
Die Zuweisung zur HaH-Behandlung der Klinik Arlesheim erfolgt in ca. der Hälfte der Patient/-innen direkt durch den Hausarzt und zu einem Viertel durch den Notfall. Eine geringe Anzahl der Patient/-innen wird aus stationärer Behandlung oder von anderen Fachärzt/-innen zugewiesen.
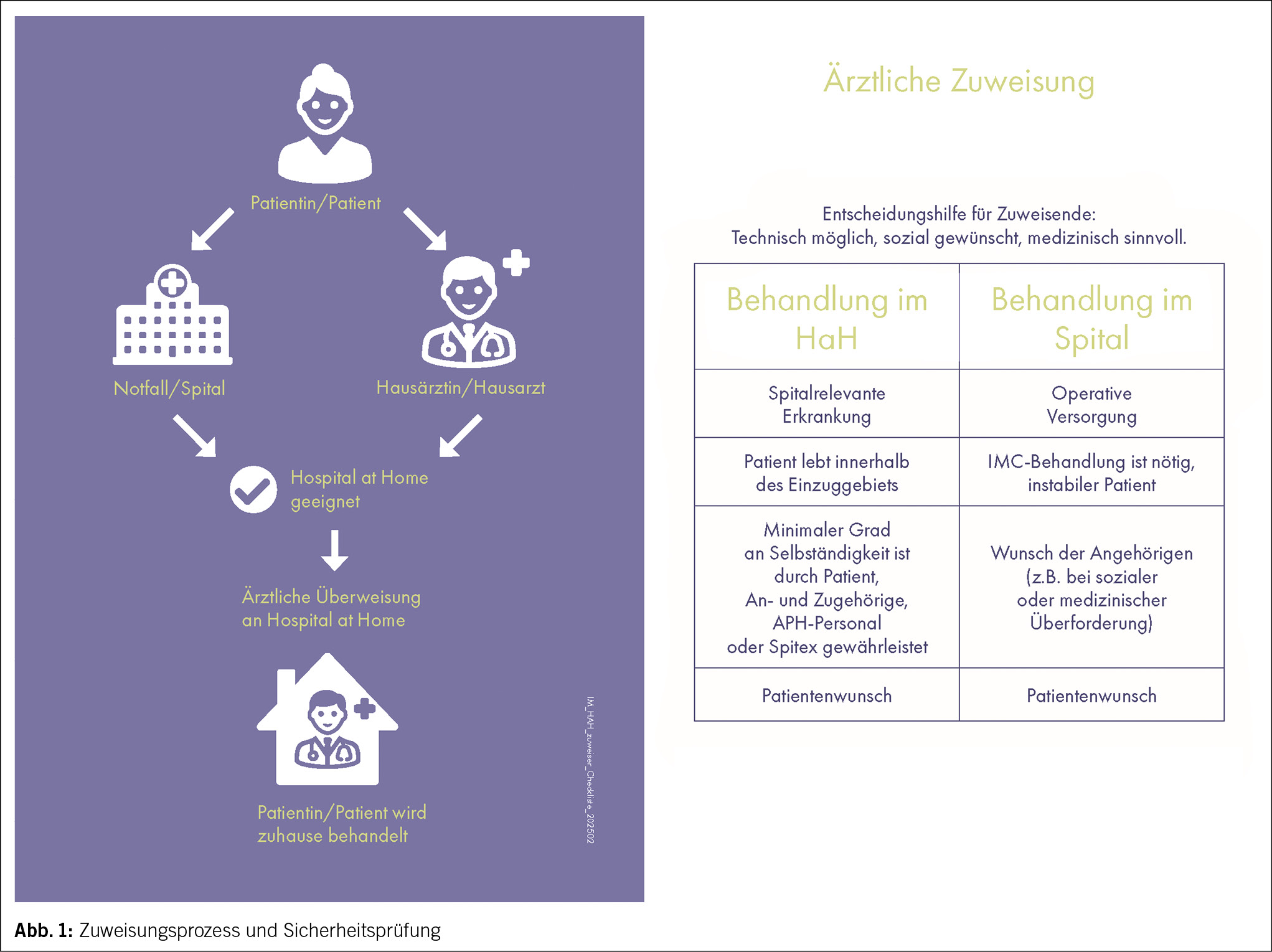
Eine Zuweisung in die HaH-Behandlung erfordert eine ärztliche Feststellung der stationären Behandlungspflichtigkeit. Anschliessend erfolgt durch das interprofessionelle Behandlungsteam eine pflegerische und ärztliche Einschätzung, ob eine HaH-Behandlung sicher durchführbar, technisch möglich, sozial erwünscht und medizinisch sinnvoll zu Hause machbar ist (Abb. 1). Die Evaluation dieser Kriterien, welche als Sicherheitsprüfung dienen, erfolgt kontinuierlich, beginnend bei der ärztlichen Zuweisung und endet mit einer abschliessenden Prüfung während der Aufnahmevisite im Zuhause der Patient/-innen. Erst im Anschluss wird ein erstes Therapiekonzept festgelegt. Weiter wird bei Bedarf das kontinuierliche Home Monitoring installiert und der/die Patient/-in wird in dessen Handhabung instruiert. Eine Aufnahme ins HaH ist von Montag bis Sonntag während 24 h möglich.
Eine Chance der neuen Versorgungsform bietet die Behandlung von besonders vulnerablen Patient/-innen in heilpädagogischen Einrichtungen sowie Alters- und Pflegeheimen. Es besteht die Möglichkeit, dass die Bewohner/-innen in ihrer Wohneinrichtung bei akuten Erkrankungen, die hausärztlich nicht mehr verantwortet und versorgt werden können, anstelle einer Spitaleinweisung durch das HaH-Team in der Wohneinrichtung behandelt werden.
Das Team von Hospital at Home kann je nach medizinisch-pflegerischen Behandlungsaufwand in der untersuchten Phase 4 bis 8 Patient/-innen gleichzeitig behandeln.
Behandlung
Das HaH-Konzept beinhaltet tägliche Visiten durch pflegerisches und ärztliches Personal. Dauer und Häufigkeit der Visiten werden in Abhängigkeit des klinischen Zustands sowie des Bedürfnisses des/der Patient/-in skaliert. Nach bisherigen Erfahrungen benötigen nur etwas über 30 % der Patient/-innen mehr als 2 Visiten pro Tag. Die Hälfte der Patient/-innen kann nach maximal 1 Woche entlassen werden.
Die Therapieintensität der Behandlung wird analog zu einem Spitalaufenthalt nach Bedarf des/der Patient/-in im Behandlungsverlauf angepasst und ständig reevaluiert. Das Equipment für Diagnostik, Therapie und Versorgung inkl. Medikamente, EKG (Elektrokardiogramm), Ultraschall, POCT(Point of Care Testing)-Labor sowie Notfallequipment werden durch das HaH-Team mitgebracht. Intensivere Untersuchungen, z. B. Magnetresonanztomografie (MRT), Computertomografie (CT), endoskopische Untersuchungen oder Echokardiografie werden, sofern notwendig, mit regionalen Gesundheitsdienstleistern durchgeführt.
Am Tag vor der Entlassung erhalten die Patient/-innen notwendige Medikamentenverschreibungen und einen Austrittsbericht. Zudem werden Termine zur weiteren ambulanten Anschlussversorgung, wie z. B. Physiotherapie oder den nächsten Termin bei dem/der Hausärzt/-in, vereinbart. Um einen nahtlosen Übergang in der ambulanten Weiterbehandlung zu gewährleisten, erfolgt die direkte Rücksprache mit dem weiterbehandelnden Team (Hausärzt/-innen, Spitex, sofern etabliert), welche auch den Austrittsbericht von der HaH-Behandlung bekommt.
Im Falle eines Notfalls oder eines dringlichen medizinischen Vorkommnisses haben Patient/-innen rund um die Uhr die Möglichkeit, das HaH-Team zu kontaktieren. Es besteht eine 24/7 h ärztliche und pflegerische Rufbereitschaft. Zur Gewährleistung einer maximalen Sicherheit der Patient/-innen erfolgt bei Bedarf ein 24/7 h telemedizinisches Monitoring der Vitalparameter (10). Nach den bisherigen Erfahrungen benötigen nur 10 % der Patient/-innen ein telemedizinisches Monitoring.
Komplikationen (z. B. Delir oder Stürze) sowie Spitalverlegungen während der HaH-Behandlung werden systematisch im Rahmen der pflegerischen und ärztlichen Betreuung erfasst.
Erste Ergebnisse
Nachfolgend werden deskriptiv die Ergebnisse aus einer retrospektiven Analyse aller 89 Patient/-innen, die zwischen dem 1. Juni 2023 und dem 31. Dezember 2023 im HaH der Klinik Arlesheim behandelt wurden, dargestellt.
Hospital at Home erreicht ein vielfältiges, geriatrisch geprägtes Patient/-innen-Kollektiv
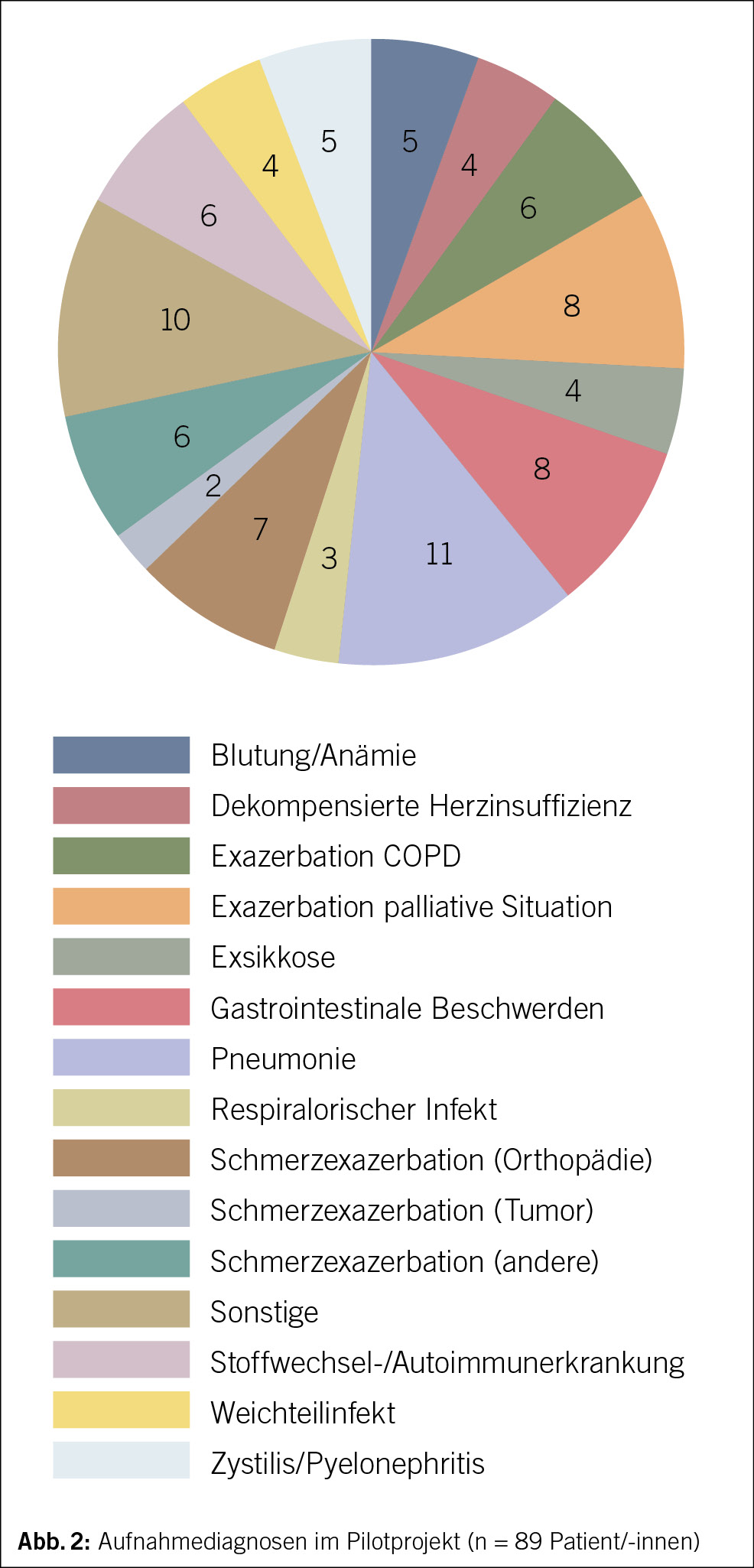
Das Alter (Standardabweichung, SD) des HaH-Kollektivs lag durchschnittlich bei 73 (± 18) Jahren (55 % weibliche Patienten). Die im HaH behandelten Diagnosen verdeutlichen das breite Spektrum an Erkrankungen, welches in diesem Versorgungsmodell behandelt werden kann (Abb. 2).
Der Mittelwert des Charlson-Komorbiditätsindex (SD), welcher das generelle Mortalitätsrisiko basierend auf der Anzahl und Schwere der Begleiterkrankungen darstellt, lag bei 2.8 (± 2.2, Range von 0–10), was einem 1-Jahres-Mortalitätsrisiko von ca. 10 % entspricht (11). 53 % der im HaH behandelten Patient/-innen wiesen einen Selbstpflegeindex (SPI) unter 32 auf (bei einem mittleren SPI [SD] von 31.9 [8.1]) (12). Der SPI (Range von 0–40) dient als Marker für die Selbständigkeit der Patient/-innen, wobei tiefere Werte einen höheren pflegerischen Aufwand bedeuten und bei Werten unter 32 weitere Schritte zur Abklärung der poststationären Versorgung einzuleiten sind. Eine Studie in 1372 Patient/-innen, die notfallmässig in die Innere Medizin des Kantonsspitals Aarau aufgenommen wurden, wies einen mittleren SPI (SD) von 35.6 (6.0) auf (13).
Diese Werte demonstrieren, dass es sich bei dem behandelten HaH-Kollektiv um polymorbide Patient/-innen mit erhöhtem Pflegeaufwand handelte.
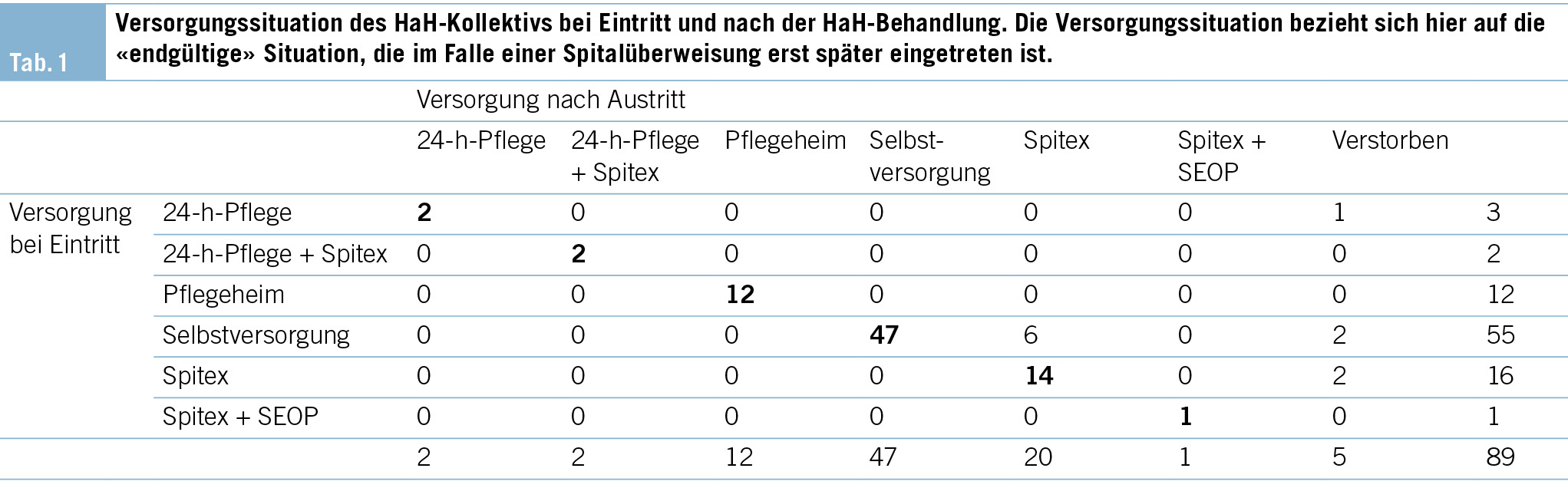
Hospital at Home ermöglicht den Verbleib in der ursprünglichen Versorgungssituation
Tab. 1 stellt die Veränderung der Versorgungssituation des Patient/-innen-Kollektivs vor und nach der HaH-Behandlung dar, wobei die Situation bei Austritt sich auf die endgültige Versorgungssituation der Patient/-innen bezieht, die bei Spitalüberweisungen erst später eintrat. Aus der Kreuztabelle wird ersichtlich, dass 78 der 89 Patient/-innen in ihrer Versorgungssituation verblieben. 6 von 55 (11 %) Patient/-innen, die sich vorher noch selbst versorgt haben, erhielten nach der Entlassung Unterstützung durch die Spitex. Nur bei 3 Patient/-innen kam es in Bezug auf die Betreuungsintensität der Spitex zu einem höheren Betreuungsbedarf als vor der HaH-Behandlung. 12 Patient/-innen wurden in einem Pflegeheim betreut und verblieben auch dort.
4 Patient/-innen verstarben, bevor sie die durch die HaH begonnene Versorgung beendet hatten, und 1 Patient starb nach vorheriger Verlegung in ein anderes Spital. Alle diese Patient/-innen befanden sich in einer palliativen Lebenssituation und wurden aufgrund dieser oder aufgrund einer zusätzlichen akuten Erkrankung zugewiesen. Zu einem unerwarteten Todesfall ist es nicht gekommen.
10 Patient/-innen wurden während der HaH-Behandlung in ein Spital überwiesen, was in 7 Patient/-innen aus medizinischen oder technischen Gründen (z. B. aufgrund einer Zustandsverschlechterung oder zur weiteren Diagnostik) notwendig war und in 3 Patient/-innen aus sozialen Gründen (häusliche Unterversorgung oder Wunsch der Patient/-innen) erfolgte. Zu einer Verlegung pflegebedürftiger Patient/-innen aus dem häuslichen Setting in die Kurz- oder Langzeitpflege kam es im HaH-Kollektiv der Klinik Arlesheim nicht. Ebenso wurde bei keinem/ keiner Patient/-in ein Bedarf für eine geriatrische Rehabilitation festgestellt.
Hospital at Home zeigt ein geringes Auftreten unerwünschter Ereignisse
Bei 3 Patient/-innen kam es unter dem HaH-Aufenthalt zu einem Sturz, was eine beobachtete Sturzrate von 4.1 Stürzen pro 1000 Pflegetagen ergibt. Laut verschiedener internationaler Studien, welche über die Sturzhäufigkeit bei stationären Patient/-innen in unterschiedlichen klinischen Populationen berichten, liegt die Sturzhäufigkeit zwischen 2.7 und 11.7 pro 1000 Pflegetagen (14–17). Die Sturzrate im HaH-Kollektiv in Arlesheim ist somit als gering bis moderat einzustufen.
Häufige spital-assoziierte Komplikationen wie Delir und nosokomiale Infektionen wurden im HaH-Kollektiv nicht beobachtet, und nur bei 2 Patient/-innen (2 %) wurde während des HaH-Aufenthaltes ein neuer Dekubitus diagnostiziert.
Hospital at Home sorgt für eine hohe Zufriedenheit der Patient/-innen und Angehörigen
Zur Erfassung der Zufriedenheit von Patient/-innen und Angehörigen verwendet die Klinik Arlesheim einen selbst entworfenen Fragebogen, welcher von 33 Patient/-innen beantwortet wurde (Rücklaufquote 37 %). Alle 33 Patient/-innen würden die Behandlung im HaH der Klinik Arlesheim weiterempfehlen und empfanden die ärztliche und pflegerische Behandlung als erstklassig (84.8 %) oder gut (15.2 %). Auch die Rückmeldungen von Angehörigen (n = 27) fielen positiv aus. Die Angehörigen fühlten sich durch die HaH-Behandlung sicher begleitet, empfanden die Zeit während der Behandlung als entlastend und fühlten sich in Entscheidungen miteinbezogen.
Zusammenfassung und Ausblick
Insgesamt gelingt es dem HaH der Klinik Arlesheim, ein geriatrisches, polymorbides Patient/-innen-Kollektiv mit erhöhtem Pflegebedarf im häuslichen Umfeld – unterstützt durch Angehörige und ambulante Pflegedienstleister – zu betreuen und so Überweisungen ins Spital zu vermeiden. Der Erhalt der Versorgungssituation trotz einer akut spitalpflichtigen Erkrankung, die geringe Häufigkeit von Dekubitus und Stürzen und das Vermeiden von Delirien und nosokomialen Infektionen sowie das positive Feedback der Patient/-innen und Angehörigen unterstreichen das Potenzial, welches im HaH-Konzept liegt, Spitaleinweisungen bei Aufrechterhaltung der Qualität zu vermeiden und so nachhaltig die Gesundheitsversorgung der Bevölkerung zu verbessern.
Neben den Möglichkeiten und Chancen der neuen Versorgungsform gehören auch Herausforderungen zur täglichen Arbeit im HaH-Modell. Dazu zählt beispielsweise der organisatorische Aufwand, den die Vorausplanung des Materials und der Medikamente in Anspruch nimmt, die für die täglichen Visiten bei den Patient/-innen benötigt werden. Auch die Entscheidungsfindung, wann eine Behandlung zu Hause mit einem zu hohen Risiko einer Verschlechterung des Gesundheitszustands für den/die Patient/-in verbunden ist und nicht mehr verantwortet werden kann, gehört zum Alltag der Gesundheitsfachpersonen. Für eine erfolgreiche Implementierung des HaH-Modells ist daher ein hohes Mass an Flexibilität und Teamarbeit erforderlich, weshalb neue Formen der interprofessionellen Zusammenarbeit über verschiedene Sektoren hinweg in Arlesheim erprobt werden.
Die erste Resonanz der Mitarbeitenden ist jedoch positiv, insbesondere durch die starke Patientenzentrierung und die enge interprofessionelle Zusammenarbeit im Behandlungsteam.
In Bezug auf die Implementierung der neuen Versorgungsform im Gesundheitswesen sehen sich die Gesundheitsfachpersonen mit der Finanzierungsfrage konfrontiert. Es werden neue Abrechnungsmodelle benötigt werden, damit die HaH-Teams kostendeckend arbeiten können. Eine systematische Evaluation von Kosten und Nutzen ist geplant, um hier zu datengestützten Entscheidungen zu kommen.
Die ersten Evaluationsergebnisse unterstützen die Annahme, dass Hospital at Home eine spitaläquivalente, sichere und qualitativ hochwertige Medizin mit einer hohen Zufriedenheit der Patient/-innen, Angehörigen und Mitarbeiter/-innen ermöglicht. Damit könnte Hospital at Home in Zukunft einen Beitrag zur Weiterentwicklung der integrierten Versorgung leisten.
Caroline Schneider 1*, Severin Pöchtrager 2, 3*, Tane Lammers 2, 3, Thomas Bürkle 4, Christiane Eberhardt 2, Philipp Busche 5, Lukas Schöb 5, Daniel Krüerke 6, Markus Singer 7, Werner Vach 8, Friederike Johanna Schirin Thilo 1
*Geteilte Erstautorenschaft
1 Berner Fachhochschule, Angewandte Forschung und Entwicklung Pflege, Department Gesundheit, Bern, Schweiz
2 Hospital at Home, Klinik Arlesheim, Arlesheim, Schweiz
3 hospitales Verein, Dornach, Schweiz
4 Berner Fachhochschule, Institut für Medizininformatik, I4MI, Departement Technik und Informatik, Biel, Schweiz
5 Innere Medizin, Klinik Arlesheim, Arlesheim, Schweiz
6 Klinik Arlesheim, Departement Forschung, Arlesheim, Schweiz
7 Palliativklinik im Park, Arlesheim, Schweiz
8 Basel Academy for Quality and Research in Medicine, Basel, Schweiz
Historie
Manuskript eingegangen: 05.12.2024
Angenommen nach Revision: 10.03.2025
Herkunft der Arbeit (Institution/Klinik)
Die Arbeit entstand aus einer Kooperation des Vereins hospitales mit der Berner Fachhochschule und Basel Academy for Quality and Research in Medicine. Die Daten der HaH-Patient/-innen stammen aus der Klinik Arlesheim.
Berner Fachhochschule, Department Gesundheit, aF & E Pflege
Murtenstrasse 10
3008 Bern
caroline.schneider@bfh.ch
Die Autorenschaft hat keine Interessenkonflikte im Zusammenhang mit diesem Artikel deklariert.
1. Kanagala SG, Gupta V, Kumawat S, Anamika F, McGillen B, Jain R. Hospital at home: emergence of a high-value model of care delivery. Egypt J Intern Med. 2023;35(1):21. https://doi.org/10.1186/s43162-023-00206-3
2. Casteli CPM, Mbemba GIC, Dumont S, Dallaire C, Juneau L, Martin E, u. a. Indicators of home-based hospitalization model and strategies for its implementation: a systematic review of reviews. Syst Rev. 2020;9:172. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7415182/
3. Vaartio-Rajalin H, Fagerström L, Santamäki-Fischer R. They Know Me and My Situation-Patients’ and Spouses’ Perceptions of Person-Centered Care in Hospital-at-Home Care. Holist Nurs Pract. 2021;35(6):332–43.
4. Mas MÀ, Santaeugènia SJ, Tarazona-Santabalbina FJ, Gámez S, Inzitari M. Effectiveness of a Hospital-at-Home Integrated Care Program as Alternative Resource for Medical Crises Care in Older Adults With Complex Chronic Conditions. Journal of the American Medical Directors Association. 2018;19(10):860–3. https://www.sciencedirect.com/science/article/pii/S1525861018303335
5. Chua CMS, Ko SQ, Lai YF, Lim YW, Shorey S. Perceptions of Hospital-at-Home Among Stakeholders: a Meta-synthesis. J Gen Intern Med. 2022;37(3):637–50. : https://doi.org/10.1007/s11606-021-07065-0
6. Anwar MM, Shamaz H, Li N, Crosbie H, Mcgeachy C, Harding A, u. a. The future of hospital at home: a qualitative interview study of healthcare staff. Eur Geriatr Med. 2024;15(4):1001–5. https://doi.org/10.1007/s41999-024-00982-3
7. González-Colom R, Carot-Sans G, Vela E, Espallargues M, Hernández C, Jiménez FX, Nicolás D, Suárez M, Torné E, Villegas-Bruguera E, Ozores F. Five years of Hospital at Home adoption in Catalonia: impact and challenges. medRxiv. 2023. https://www.medrxiv.org/content/10.1101/2023.01.25.23284997v2
8. Edgar K, Iliffe S, Doll HA, Clarke MJ, Gonçalves-Bradley DC, Wong E, u. a. Admission avoidance hospital at home. Cochrane Database of Systematic Reviews, 2024 (3). https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD007491.pub3/full
9. Koechlin S. Arztvisite zuhause. Schweizerische Ärztezeitung 2024 [zitiert 27. November 2024]. Verfügbar unter: https://saez.swisshealthweb.ch/de/article/doi/saez.2024.1253151792
10.Poechtrager S, Goetz T, Heider S, Kirchner N, Müller C E. Gut behandelt zuhause. Schweizerische Ärztezeitung 2024 [zitiert 27. November 2024]. Verfügbar unter: https://saez.swisshealthweb.ch/de/article/doi/saez.2023.21128/
11.Bannay A, Chaignot C, Blotière PO, Basson M, Weill A, Ricordeau P, u. a. The Best Use of the Charlson Comorbidity Index With Electronic Health Care Database to Predict Mortality. Med Care. 2016;54(2):188–94. DOI: 10.1097/MLR.000000000000047
12.eP Handbuch ePA-AC 2, Wiesbaden.
13.Conca A, Koch D, Regez K, Kutz A, Haubitz S, Schuetz P, u. a. Extension and Validation of the Self-care Index to Predict Transfer to a Post-acute Care Institution in Internal Medicine Patients. International Journal of Health Professions. 2022;9(1):59–66.: https://www.sciendo.com/article/10.2478/ijhp-2022-0005
14.Halfon P, Eggli Y, Van Melle G, Vagnair A. Risk of falls for hospitalized patients: A predictive model based on routinely available data. Journal of Clinical Epidemiology. 2001;54(12):1258–66. https://www.sciencedirect.com/science/article/pii/S0895435601004061
15.Schwendimann R, Bühler H, De Geest S, Milisen K. Falls and consequent injuries in hospitalized patients: effects of an interdisciplinary falls prevention program. BMC Health Services Research. 2006; 6(1):69. https://doi.org/10.1186/1472-6963-6-69
16.Visvanathan R, Ranasinghe DC, Lange K, Wilson A, Dollard J, Boyle E, u. a. Effectiveness of the Wearable Sensor-based Ambient Intelligent Geriatric Management (AmbIGeM) System in Preventing Falls in Older People in Hospitals. The Journals of Gerontology: Series A 2022; 77(1):155–63. https://doi.org/10.1093/gerona/glab174
17.von Renteln-Kruse W, Krause T. Sturzereignisse stationärer geriatrischer Patienten. Zeitschrift für Gerontologie und Geriatrie. 2004;37(1):9–14. https://doi.org/10.1007/s00391-004-0204-7