La prévalence de l’ hypertension artérielle augmente avec l’ âge, atteignant 60% chez les patients de plus de 60 ans, et 75 % à plus de 75 ans. Selon les dernières recommandations des Sociétés Européennes de Cardiologie et d’ Hypertension (ESC/ESH) pour la prise en charge de l’ hypertension artérielle (1), une personne est définie comme âgée à > 65 ans et très âgée à > 80 ans.
Existe-t-il un bénéfice à un traitement antihypertenseur ?
Pendant plusieurs années, l’ âge avancé a été un obstacle dans le traitement de l’ hypertension de la personne âgée, en raison de craintes concernant une faible tolérance au traitement et d’ effets indésirables. Certains rapports ont suggéré que les interventions visant à normaliser la tension artérielle (TA) peuvent provoquer une dysfonction d’ organes. Cette appréciation est inappropriée, car l’ évidence émanant d’ études randomisées et contrôlées (RCT) montre que le traitement anti-hypertenseur chez la personne âgée et très âgée diminue la morbidité et la mortalité cardiovasculaires, ainsi que la mortalité de toute cause (2). Finalement, le traitement de l’ hypertension artérielle est en général bien toléré.
Comorbidités, fragilité, et traitement anti-hypertenseur
Toutefois, les patients âgés présentent souvent des comorbidités telles qu’ une insuffisance rénale, une vasculopathie athérosclérotique et une hypotension orthostatique, qui peuvent toutes être aggravées par l’ instauration d’ un traitement anti-hypertenseur. La polymédication peut également constituer une limitation majeure, des interactions médicamenteuses pouvant augmenter le risque d’ effets indésirables des traitements anti-hypertenseurs. Plus important encore, les patients très fragiles, dépendants et ceux présentant une hypotension orthostatique n’ ont pas été inclus dans les études randomisées et contrôlées ayant testé l’ effet des traitements anti-hypertenseurs. Le bénéfice de ces traitements dans le contexte des comorbidités et d’ une espérance de vie réduite est dès lors incertain. En conséquence, le patient âgé avec une hypertension artérielle est souvent plus difficile à traiter qu’ un patient jeune, car la décision d’ initier un traitement doit tenir compte de sa fragilité, de ses comorbidités et des traitements concomitants.
Traitement antihypertenseur chez le patient âgé
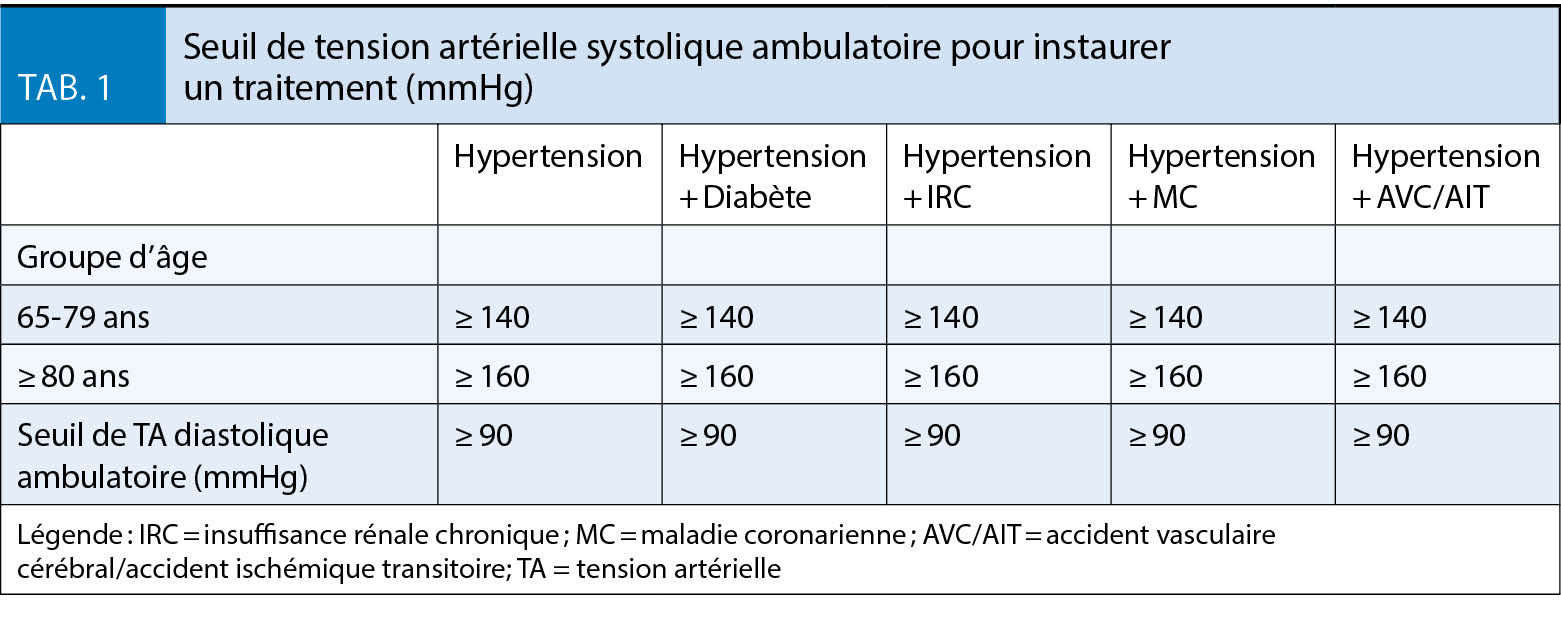
L’ âge ne doit jamais être le seul argument en défaveur d’ un traitement anti-hypertenseur, car une TA élevée est un facteur de risque cardiovasculaire important, y compris chez la personne très âgée. Une récente étude a montré une réduction du risque d’ événements cardiovasculaires et de la mortalité après instauration d’ un traitement antihypertenseur, y compris chez les patients de plus de 85 ans dans une population générale, incluant également des patients fragiles (3). Les directives internationales recommandent donc l’ initiation d’ un traitement quand la TA est au-dessus du seuil indiqué dans la Figure 1. En général, une monothérapie semble appropriée chez le patient très âgé. Toutefois, un traitement combiné est possible chez le patient âgé, mais chaque molécule devrait être débuté à la dose la plus basse disponible.
Eléments à considérer dans le traitement anti-hypertenseur
En raison du risque associé à l’ hypotension orthostatique, cette complication doit être recherchée, en particulier chez le patient sous traitement antihypertenseur présentant des symptômes compatibles avec des épisodes hypotensifs non-reproductibles durant la consultation. Il est à noter que les diurétiques de l’ anse et les alpha-bloqueurs devraient être évités, sauf en cas d’ indication autre, en raison de leur association avec les chutes (4). Finalement, la fonction rénale doit être évaluée fréquemment à la recherche d’ une péjoration de la fonction rénale pouvant être induite par une diminution de la perfusion rénale. Si toléré, la TA doit être abaissée à des valeurs systoliques de 130-139 mmHg et diastoliques de < 80 mmHg. Une valeur systolique de < 130 mmHg doit être évitée (1).
Une attention particulière doit être apportée à la recherche d’ effets secondaires et de problèmes de tolérance associés au traitement hypertenseur de la personne âgée, et plus particulièrement de la personne très âgée. Ces complications surviennent de manière plus fréquente chez les personnes âgées que rapporté dans les essais cliniques randomisés, et imposent donc une expertise spécialisée et un suivi rapproché visant à les minimiser.
Une problématique importante est l’ hypotension orthostatique de la personne très âgée et fragile et dépendante, profil fréquemment exclu des RCT. Toutefois, l’ étude SPRINT a montré que le bénéfice d’ une réduction de la pression artérielle s’ étend aussi aux personnes âgées fragiles, et celles avec une vitesse de déplacement réduite (5), et non pas uniquement aux personnes âgées en relatif bon état de santé. Il faut finalement noter que la magnitude du bénéfice d’ un tel traitement chez la personne âgée très fragile et institutionnalisée est inconnue. Chez certains patients, la valeur tensionnelle la plus adéquate peut être plus élevée que les cibles recommandées, mais il doit être reconnu que chaque décrément de tension artérielle apporte probablement un bénéfice ainsi qu’ une réduction du risque d’ événements cardiovasculaires majeurs (en particulier celui d’ AVC et d’ insuffisance cardiaque) et de mortalité.
Dr Nicolas Barras Dr Tamila Abdurashidova Dr Patrick Yerly Dr Julien Regamey
Pr Roger Hullin
CHUV, Service de Cardiologie
Département Cœur-Vaisseaux
Rue du Bugnon 44
1011 Lausanne
roger.hullin@chuv.ch
Les auteurs ont déclaré n’avoir aucun conflit d’ intérêts en relation avec cet article.
L’ évidence émanant d’ études randomisées et contrôlées (RCT) montre que le traitement anti-hypertenseur chez la personne âgée et très âgée diminue la morbidité et la mortalité cardiovasculaires, ainsi que la mortalité de toute cause.
Le patient âgé avec une hypertension artérielle est souvent plus difficile à traiter qu’ un patient jeune, car la décision d’ initier un traitement doit tenir compte de sa fragilité, de ses comorbidités et des traitements concomitants.
Une attention particulière doit être apportée à la recherche d’ effets secondaires et de problèmes de tolérance associés au traitement hypertenseur de la personne âgée, et plus particulièrement de la
personne très âgée.
1. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. ESC/ESH Guidelines for the management of arterial hypertension. European Heart J 2018, 39 :3021-3014.
2. Beckett NS, Peters R, Fletcher AE, Staessen JA, Liu L, Dumitrascu D, et al. HYVET Study Group. Treatment of hypertension in patients 80 years of age or older. N Engl J Med 2008;358:1887-1898.
3. Corrao G, Rea F, Monzio Compagnoni M, Merlino L, Mancia G. Protective effects of antihypertensive treatment in patients aged 85 years or older. J Hypertens 2017;35:1432-1441.
4. Corrao G, Mazzola P, Monzio Compagnoni M, Rea F, Merlino L, et al.. Antihypertensive medications, loop diuretics, and risk of hip fracture in the elderly: a population-based cohort study of 81,617 Italian patients newly treated between 2005 and 2009. Drugs Aging 2015;32:927-936.
5. Williamson JD, Supiano MA, Applegate WB, Berlowitz DR, Campbell RC, Chertow GM, et al. SPRINT Research Group. Intensive vs standard blood pressure control and cardiovascular disease outcomes in adults aged >_75 years: a randomized clinical trial. JAMA 2016;315:2673–2682.
Les abcès et les fistules ano-rectales entrent dans le groupe des pathologies proctologiques fréquemment rencontrées. Leur incidence est de 2 cas sur 10 000 habitants. Elles doivent être connues du praticien qui est en mesure d’en faire le diagnostic et d’initier la prise en charge sans délais. Cet article aborde le traitement des abcès anaux et des fistules ano-rectales.
Pour la petite histoire
Le roi-soleil Louis XIV souffrait de crises récidivantes de maladie fistuleuse ano-rectale. Les médecins du Roy, à leur tête Antoine Daquin, impuissants à le traiter firent appel au barbier Charles François Félix. Ils étudièrent et planifièrent une section directe de la fistule à l’ aide d’ un fistulotome inspiré de méthodes italiennes. Après une période d’ essais « cliniques» auprès de condamnés de la Bastille et de volontaires, l’ intervention de la fistule royale eut lieu le 18 novembre 1696 et le roi soleil fut débarrassé définitivement de sa maladie fistuleuse. En guise de récompense, outre de riches présents octroyés par Louis XIV, Louis XV son petit fils créa « la royale académie chirurgicale» et donna ainsi ses lettres de noblesse à la confrérie des barbiers, tant décriés par les Médecins du Roy. Pour rendre grâce à cette guérison Lulli composa un hymne « Grand Dieu sauve le Roy » qui fut repris 28 ans plus tard par Haendel et devint le God save the King (Queen) hymne national Anglais actuel.
La fréquence des abcès anaux et des fistules est élevée. Ils surviennent de préférence chez l’ homme jeune. Ces pathologies trouvent leur origine au niveau des glandes anales situées dans l’ espace inter-sphinctérien. Leur classification dépend de leur localisation par rapport aux sphincters de l’ anus. L’ histoire de la maladie et l’ examen clinique du patient suffisent en général à poser le diagnostic et élaborer le traitement chirurgical. Des investigations complémentaires (endoscopie, endosonographie, résonance magnétique) sont utiles en cas d’ abcès ou de fistules complexes. Le but de la chirurgie lors d’ abcès est de drainer l’ infection tout en préservant l’ intégrité anatomique des sphincters. Le risque de récidive de l’ abcès ou son évolution vers une fistule est limité. Il peut résulter d’ un drainage insuffisant. Le traitement de la fistule dans le même temps du drainage de l’ abcès est réservé aux fistules superficielles qui n’ interférent pas avec le sphincter. Il doit être réalisé par un chirurgien expérimenté. Tous les autres types de fistules doivent être traités en un second temps. Le traitement de la fistule est chirurgical il peut être réalisé, en fonction du type de la fistule par les techniques suivantes :
Drainage par fil de séton, fistulotomie, fistulectomie
Plastie et reconstruction du sphincter (sphinctéroplastie, lambeau muqueux, LIFT), techniques endo luminales (VAAFT)
Techniques d’ occlusion (fibrine, plug, clip, laser…).
Seules les fistules dont le trajet est distal peuvent être traitées par fistulotomie ou fistulectomie. Toutes les fistules hautes doivent bénéficier d’ une technique protégeant le sphincter et par la même la continence du patient. Les résultats des différentes techniques de reconstruction et de plastie du sphincter sont superposables. Les techniques d’ occlusions sont grevées d’ un taux de récidive plus élevé. Notre propos s’ attachera à donner les clés du diagnostic et du traitement des abcès et des fistules basé sur notre expérience et la revue de la littérature.
Les abcès ano-rectaux et les fistules anales sont parmi les pathologies les plus fréquemment rencontrées en pratique proctologique. Leur incidence est de 2 cas par 10 000 habitants. Elles doivent être connues du praticien qui est parfaitement à même d’ en initier le traitement (1).
L’ abcès ano-rectal et la fistule anale sont deux entités mentionnées souvent séparément. Elles représentent en fait les phases successives d’ une même pathologie, la maladie fistuleuse ano-rectale (2).
Etiologie
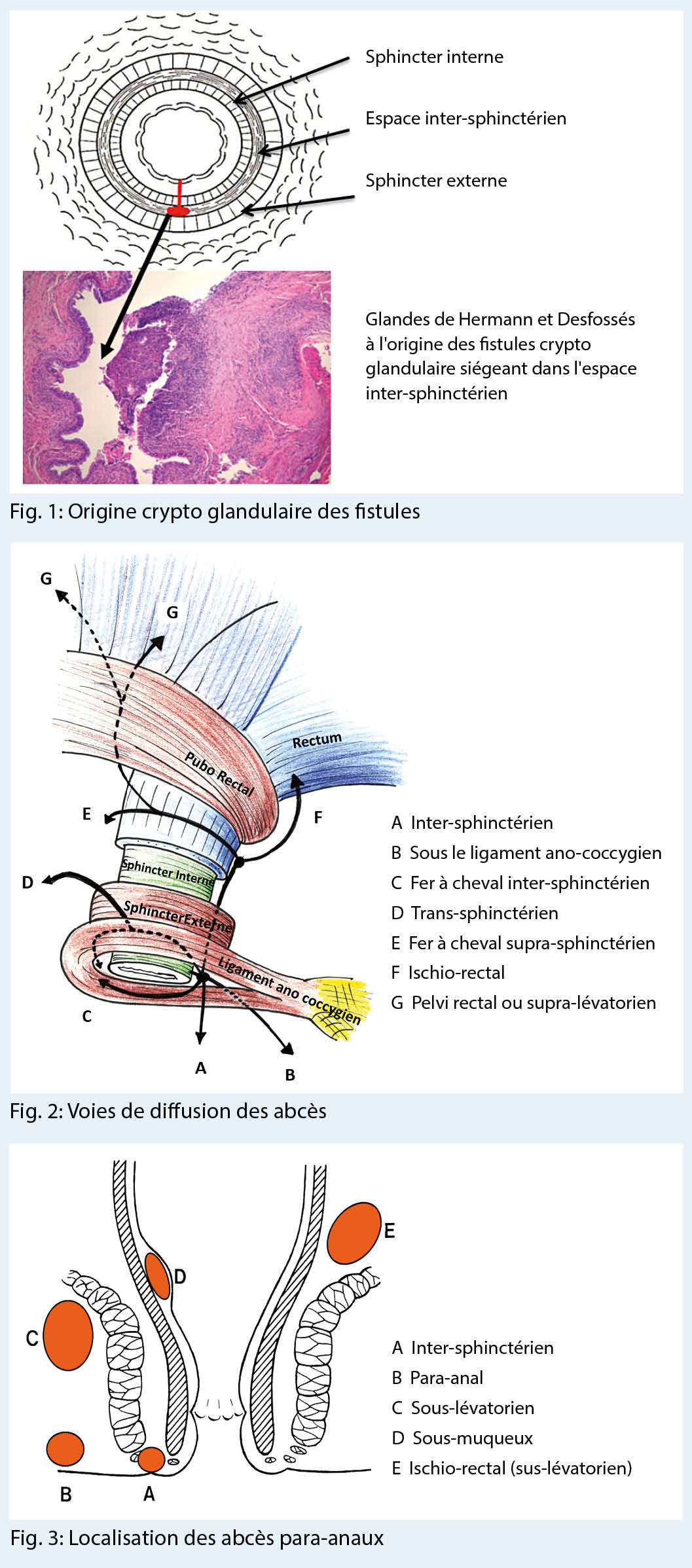
La majorité des abcès et des fistules anales (90 %) sont d’ origine crypto-glandulaire. La maladie débute dans une des glandes lubrificatrices d’ Hermann et Desfossés situées dans l’ espace inter-sphinctérien de l’ appareil sphinctérien, suite à la diminution ou l’ abolition du drainage glandulaire (Fig. 1) (3).
L’ infection glandulaire évolue rapidement en abcès à germes intestinaux et se draine dans les espaces périanaux et périnéaux de moindre résistance. Comme l’ homme a plus de glandes lubrificatrices que la femme la maladie fistulaire est plus fréquente chez l’ homme entre 30 et 50 ans dans un ratio 2/3 – 1/3 (1, 4).
Certains facteurs favorisants la venue de ces abcès ont été décrits comme le diabète, l’ obésité, l’ alcoolisme et le tabagisme (5, 6). De même la station assise prolongée, le sédentarisme, les poussées lors de la défécation et le stress psychosocial sont considérés comme facteur de risques par certains auteurs (7, 8).
Cette phase aiguë de la maladie fistuleuse crypto-glandulaire doit être différenciée d’ un abcès compliquant une maladie sous-jacente. Parmi ces abcédations dites secondaires, il faut mentionner les abcès liés à une fissure, à une hidrosadénite suppurée (maladie des glandes apocrines), à l’ infection d’ une glande sébacée, à un sinus pilonidal proche de l’ anus ou à une infection sexuellement transmise ano-rectale. En présence de récidive ou de trajets fistuleux multiples, la question d’ une maladie de Crohn sous-jacente doit être posée et la maladie inflammatoire recherchée. Finalement, les abcès compliquent fréquemment les plaies traumatiques ano-rectales (lésion sur corps étranger, plaie pénétrante, lésion iatrogène chirurgicale, obstétricale ou endoscopique) et peuvent être difficiles à relier à leur cause, en particulier si celles-ci sont ignorées ou occultées volontairement par le patient à son médecin (Tab. 1).
Voies de dissémination
L’ extension et les voies de drainage spontané des abcès de la région ano-rectale sont régies par les lois des pressions. Aux structures fermes s’ opposent des zones de moindre résistance, créant ainsi des voies de facilitation de la dissémination de l’ infection. Pour mieux le comprendre, l’ image d’ un labyrinthe peut être empruntée. Les cloisons sont le muscle sphincter interne, le muscle sphincter externe, le raphé ano-coccygien et le muscle releveur de l’ anus.
L’ abcès situé à l’ origine dans l’ espace inter-sphinctérien est guidé par les structures à haute résistance et peut diffuser soit distalement dans la région para-anale, soit proximalement dans l’ espace pelvi-rectal, au-dessus des muscles élévateurs de l’ anus, soit à travers le muscle sphinctérien externe en direction de la fosse ischio-rectale ou plus superficiellement vers le périnée (Fig. 2.)
L’ abcès tout d’ abord inter-sphinctérien évolue ainsi respectivement en abcès para-anal, pelvi-rectal, ischio-rectal ou périnéal (Fig. 3).
L’ abcès en fer à cheval se développe postérieurement au-dessus du raphé ano-coccygien. Il diffuse bilatéralement en direction des deux fosses ischio-rectales (9). Les abcès para-anaux et périnéaux représentent environ 50 % des cas, les abcès ischio-rectaux 25 %.
Tableau clinique des abcès ano-rectaux
Les symptômes cardinaux classiques des abcès ano-rectaux sont les mêmes que ceux de toute pathologie infectieuse abcédée. Ils associent douleur, rougeur, tuméfaction et chaleur. Les douleurs sont intenses et pulsatiles, stimulées par la position assise, la marche ou la défécation. Lorsque la collection est périnéale ou péri-anale, une induration palpable de la fesse apparaît. Un certain degré de cellulite d’ accompagnement peut exister. La prise en charge de ces abcès est une urgence chirurgicale.
La fièvre, parfois associée à des frissons est souvent retrouvée et ceci d’ autant plus que la lésion est haut située et donc de diagnostic plus difficile. L’ examen clinique et l’ anuscopie ne permettent d’ identifier l’ orifice interne primaire que dans 30 à 40 % des cas (2).
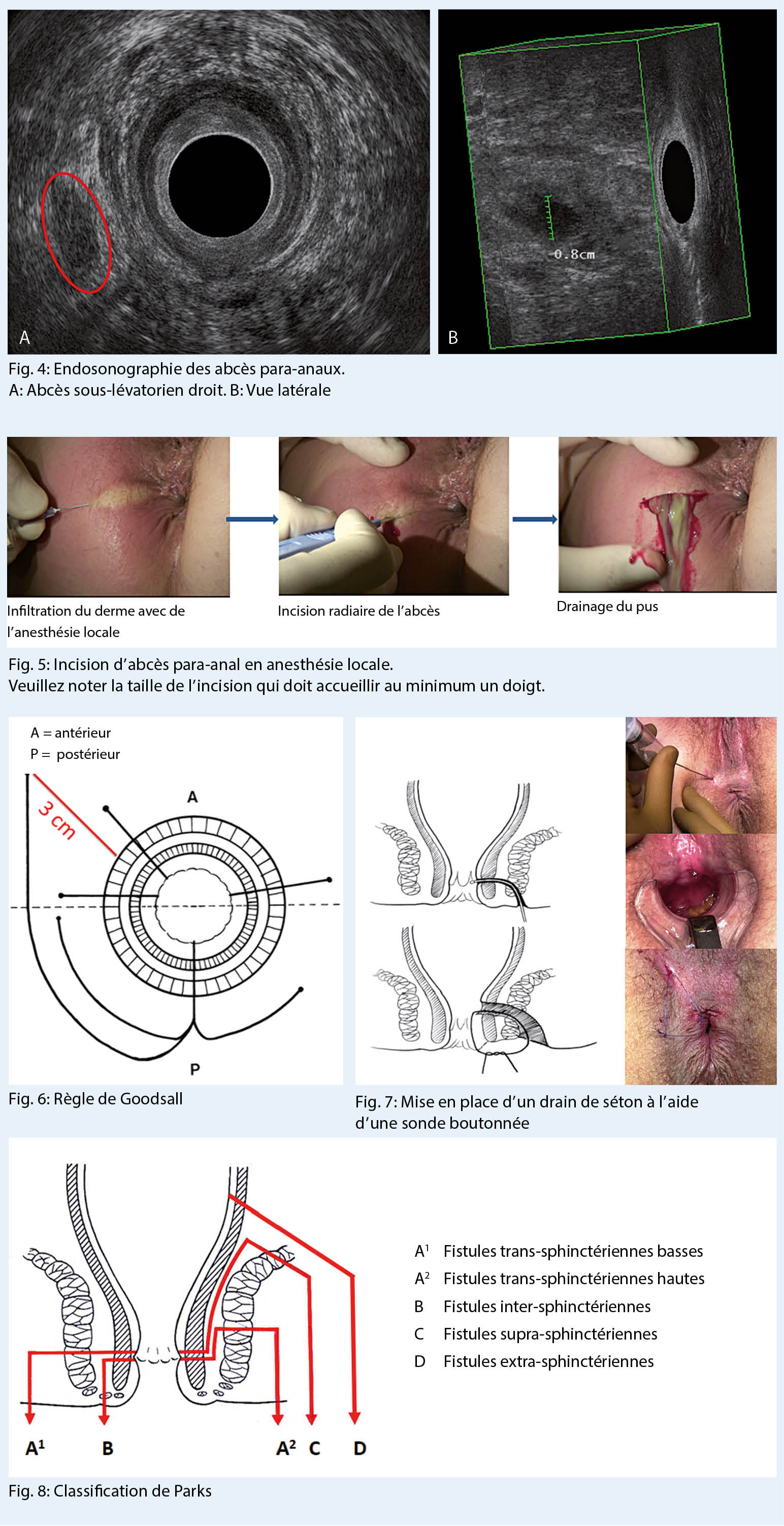
L’ abcès inter-sphinctérien reste un défi diagnostique du fait de l’ absence de signes cliniques extérieurs associé à des douleurs aiguës rendant tout examen anuscopique impossible. Celui-ci peut être réalisé sous anesthésie générale et laissera palper une petite voussure de la taille d’ un grain de riz dans l’ espace inter-sphinctérien. L’ échographie endoanale est une aide diagnostique appréciable dans ces situations, elle permet également de diriger l’ incision de drainage (Fig. 4) (10).
Si l’ abcédation n’ est pas prise en charge rapidement, le tableau clinique peut se compliquer et évoluer vers un sepsis sévère, dont il faut se rappeler l’ importante mortalité chez les patients fragiles (11). Une cellulo-fascéite anaérobie du périnée ou des bourses, nommée alors gangrène de Fournier (12, 13) représente un autre mode de complication septique gravissime, qui nécessitera un débridement agressif en extrême urgence avec parfois nécessité à confectionner une colostomie de décharge temporaire (14). Le spectre de telles complications nous rappelle la nécessité de traiter adéquatement et dans l’ urgence non différée tout abcès de la région ano-rectale.
Traitement de la maladie fistuleuse abcédée
Les abcès de la région périnéale et ano-rectale évoluent lentement et difficilement vers un drainage spontané à l’ issue d’ un trajet plus ou moins complexe. En règle générale, ils ne peuvent pas se résoudre d’ eux-mêmes spontanément. La base du traitement est le drainage chirurgical dirigé de la cavité abcédée. La recherche du trajet fistuleux d’ amont ne doit se faire que dans la deuxième phase lors du traitement de la fistule ano-rectale.
Une antibiothérapie seule est insuffisante à la guérison de l’ abcès, toujours présent dans la maladie fistulaire. Elle tend à chroniciser l’ infection et de ce fait à rendre plus complexe le drainage chirurgical (15).
Principe du drainage de l’ abcès
L’ incision est menée assez largement pour assurer un bon drainage et éviter une rétention du pus dans la poche abcédée (principe du sablier). Ceci aboutirait à un retard de la guérison, une fermeture précoce de la plaie opératoire, une persistance de l’ abcès. Elle est radiaire dans tous les cas. La recherche de tractus fistuleux et de l’ orifice primaire doit être évitée à la phase aiguë en raison du risque de fausses routes, dues à la déliquescence des tissus. Même l’ effondrement des cloisons et le curetage ne sont pas recommandés. Un lavage au sérum physiologique à la seringue est amplement suffisant. Une mèche à but hémostatique sera mise en place pour les premières 12 à 24 heures. Le traitement des abcès ano-rectaux a la particularité de pouvoir être pratiqué en anesthésie locale, sans couverture antibiotique et sans mise en culture du pus.
Nous avons l’ habitude d’ inciser les abcès para-anaux et périnéaux, qui sont les plus fréquents, en anesthésie locale et selon un mode ambulatoire. Une infiltration douce du derme qui contient les terminaisons nerveuses, par un anesthésique local tamponné par du bicarbonate (lidocaïne 0.5 % 10ml plus NaBic 0.8 mmol 1ml) en regard de l’ abcès et une incision radiaire sans pression assurent une antalgie suffisante (Fig. 5).
L’ incision d’ un abcès intersphinctérien sera menée avec prudence et avec le plus grand respect des sphincters. Les abcès sus-lévatoriens, ischio-rectaux haut placés et les abcès en fer à cheval requièrent une anesthésie générale ou péridurale.
L’ utilisation systématique d’ an-tibiotiques n’ est pas recommandée, puisqu’ il ne s’ agit pas d’ un traitement causal, celui-ci reposant sur le vieil adage « ubi pus ibi evacua». L’ introduction d’ un traitement antibactérien doit être discutée cependant, dans les contextes de patients fragilisés, immuno supprimés ou porteurs de valve cardiaque. Les germes habituellement retrouvés en culture sont des souches intestinales classiques. La mise en culture du pus n’ est donc pas utile de routine, elle sera impérative et dirigée lors de suspicion d’ infections sexuellement transmissible.
Les soins locaux
Ils doivent être facilités. La mèche est retirée par le malade lui-même le lendemain de l’ intervention et un rinçage de la plaie opératoire par douche anale pluriquotidienne est prescrit. Des antalgiques à base de paracétamol et d’ anti-inflammatoires à dose dégressive sont prescrits. La plaie est contrôlée à 24-48 heures puis de manière hebdomadaire.
Le bilan intermédiaire
4 à 6 semaines après l’ incision et après guérison de la maladie abcédée, à distance de la phase aiguë sensible, il est important de faire un bilan de la maladie fistuleuse résiduelle. Dans 25 % des cas environ, on constate la fermeture de l’ orifice secondaire, la disparition de la fistule et l’ absence d’ orifice primaire résiduel (16, 17). Dans les autres cas, l’ examen anal et rectal soigneux retrouvent l’ orifice glandulaire primaire, sous la forme d’ une caroncule palpable, de la taille d’ un grain de riz. L’ anuscopie en permettra souvent le repérage visuel. Il est important d’ exclure à ce stade toute autre pathologie du canal anal, en particulier un cancer ano-rectal abcédé.
Tableau clinique des fistules ano-rectales constituées
Les plaintes principales du patient porteur d’ une fistule anale constituée sont des écoulements para-anaux ou mal localisés du siège, salissant régulièrement les sous-vêtements. Un prurit d’ irritation péri-anal est parfois associé. Les écoulements sont classiquement intermittents. Ils sont rythmés par la séquence : occlusion du tractus fistulaire – micro-abcédation douloureuse – libération purulente à l’ orifice secondaire – écoulements et disparition des douleurs. Les problèmes d’ hygiène peuvent devenir handicapants, en particulier lorsque les orifices secondaires se multiplient au cours d’ une maladie fistulaire non traitée ou d’ une maladie de Crohn.
En cas de trajet fistuleux persistant, et à la seule inspection, la règle de Goodsall garde toute sa valeur dans la prédiction de la localisation de l’ orifice primaire situé à la ligne pectinée en fonction de l’ endroit de drainage cutané secondaire. Les tractus fistuleux drainés antérieurement sont plutôt linéaires, tandis que les trajets postérieurs sont curvilignes. Un trajet antérieur à plus de 3 cm de la marge anale peut trouver son origine dans la portion postérieure du canal anal (Fig. 6).
La palpation retrouve souvent un cordon fistuleux entre pouce et index. L’ anuscopie recherche l’ orifice primaire sous forme d’ une ombilication muqueuse ou de la présence de tissu de granulation.
Toute fistule constituée fera l’ objet d’ une tentative de mise en place d’ un drainage de séton constitué d’ un double monofilament de 4.0 ou 5.0.
Une aiguille boutonnée sera conduite dans le canal anal depuis l’ orifice secondaire avec précaution et sans pression afin d’ éviter toute fausse route.
Nous utilisons de l’ air pulsé à la seringue pour ouvrir le trajet et en repérer la perméabilité sous forme de bulles apparaissant à l’ orifice primaire. Les fils de séton lâches permettent un drainage prolongé et renforcent ainsi la fibrose péri-fistulaire. Ils peuvent être laissés en place de manière prolongée de plusieurs mois à plusieurs années, comme dans le cas particulier de la maladie de Crohn (Fig. 7).
Le repérage ultra-sonographique des trajets fistuleux aidé de l’ examen 3D, peut être utile dans le cas particulier des fistules complexes ou récidivantes (18, 19). Il peut éventuellement être associé à une IRM du petit bassin, à la recherche d’ une lésion pelvienne.
Dans des mains expertes, ces 2 examens ont une précision diagnostique comparable (20). Notre préférence va à l’ échographie endoanale 3D que nous considérons comme partie intégrante de l’ examen d’ une fistule avec pour avantage une réponse pendant la consultation et un coût inférieur.
L’ examen clinique aidé de l’ endosonographie 3D ou de l’ IRM permet de classifier les fistules. La classification la plus utile et la plus utilisée est celle de Parks (21) (Fig. 8).
Elle permet d’ associer le type de fistule à un choix de traitement chirurgical en fonction de la quantité de sphincter inclus dans le trajet. Pour l’ école genevoise, les trajets distaux peuvent être traités par l’ ablation de la fistule avec section du sphincter. Les trajets hauts doivent être traités par des techniques respectant le sphincter. Les fistules inter-sphinctériennes et trans-sphinctériennes distales re-
présentent entre 50 et 60 % des cas et les fistules trans-sphinc-tériennes hautes 25 %.
Traitement des fistules ano-rectales
Le but du traitement de la fistule ano-rectale est l’ excision du tractus fistuleux fibreux qui emporte la glande responsable de la fistule, des tractus fistuleux accessoires, la suppression de l’ orifice primaire, la préservation de la fonction anale par protection du capital sensitif et musculaire.
On peut considérer trois groupes de traitement chirurgicaux Les chirurgies avec section du sphincter
Séton tracteur, séton chimique, Fistulotomie, Fistulectomie Les chirurgies avec respect des sphincters avec ablation du trajet fistuleux
Fistulectomie et reconstruction du sphincter, Lambeau d’ avancement, LIFT technique Nouvelles méthodes par occlusion du trajet fistuleux
Laser, VAAFT, OTSC clip, Colle de fibrine, Injection de collagène, Injection de cellules germinale autologues, plug.
Les récidives restent cependant nombreuses malgré le développement récent de nouvelles techniques chirurgicales. Les traitements les plus pratiqués dans notre clinique sont la fistulotomie, la fistulectomie, le lambeau d’ avancement et l’ encollage fistulaire en fonction du type de fistule rencontré.
Les traitements classiques
Séton tracteur ou chimique
Cette technique déjà connue de l’ antiquité et rapportée par Hippocrate (22) a pour but la section progressive du sphincter compris entre la fistule et la peau. Cette section est due soit à la pression du fil soit à une destruction chimique par les composants phytothérapiques du séton (Kshara Sutra).
Si on observe une guérison de la fistule dans 80 à 100 % des cas, le taux d’ incontinence anale rapportée varie de 0 à 92 % ce qui est largement inacceptable (23, 24). Pour cette raison évidente le traitement de fistule par section progressive est abandonnée dans notre service.
Fistulotomie
La fistulotomie consiste en la mise à plat et au curetage du « tunnel fistuleux». Cette technique est réservée aux trajets muco-cutanés ou très distaux qui ne touchent pas les fibres musculaires sphinctériennes. Dans ce cas, la guérison est obtenue dans pratiquement 84 % des cas avec un taux de continence et une qualité de vie comparables à celui de la population générale (25).
Fistulectomie avec ou sans reconstruction du sphincter
Par fistulectomie, on entend l’ excision complète de l’ ensemble du trajet fistuleux et de son orifice primaire. Le revêtement cutané qui couvre la fistule est excisé avec le cordon fistuleux et la guérison se fait per secundam. Le muscle sphincter est sectionné à minima et peut être reconstruit par suture directe en cas de nécessité (26). Cette technique s’ applique aux fistules les plus distales, et de préférence postérieures. C’ est à dire les fistules périnéales, inter-sphinctériennes ou trans-sphinctériennes distales. Cette intervention peut être pratiquée en anesthésie locale parfois sur un mode ambulatoire. Dans notre expérience de 983 cas consécutifs revus de 2010 à 2018, 5.2 % des patients ont récidivé et aucun cas d’ incontinence majeure n’ est à signaler. Notre expérience est superposable aux résultats de la littérature qui démontrent un succès dans 93 % des cas avec 12 % de troubles de la continence mineurs aux gaz occasionnellement (27).
Lambeau d’ abaissement rectal (LAR)
Le traitement des fistules ano-rectales hautes ou antérieures chez la femme représente un risque pour les structures sphinctériennes et par voie de conséquence peut être grevé d’ un taux non négligeable d’ incontinence anale postopératoire.
La technique du lambeau d’ abaissement muqueux est une approche chirurgicale élégante pour les cures de fistules hautes situées dans le canal anal. Elle permet de préserver un maximum de tissu de l’ appareil sphinctérien. Elle s’ adresse donc aux fistules trans sphinctériennes hautes et aux fistules supra ou extra-sphinctériennes.
L’ excision des fistules n’ est possible qu’ en terrain calme, en présence de tractus devenus fibreux et si possible drainés par un fil de séton. L’ abaissement muqueux nécessite également un tissu parfaitement sain. Après libération d’ un lambeau de muqueuse, cette dernière est suturée sans tension et sans risque d’ ischémie. Une inflammation aiguë, un terrain post-radique, une maladie de Crohn ou néoplasique, ainsi que des forces de tension sur la ligne de suture sont voués à l’ échec de la technique.
Cette intervention est menée sous antibioprophylaxie sans préparation intestinale, ni rasage préopératoire. Une stomie d’ amont n’ est jamais réalisée.
Le premier temps opératoire consiste en l’ excision complète du trajet fistuleux qui est menée progressivement à partir de l’ orifice secondaire par une dissection au contact du tractus fibreux jusqu’ à l’ orifice interne. Cette dissection réalise alors un « carottage» trans sphinctérien qui vise à n’ emporter idéalement que le tractus fibreux en respectant le tissu musculaire. Une collerette de muqueuse anale autour de l’ orifice primaire est également excisée. Le deuxième temps réalise la fermeture musculaire, par des points séparés d’ un mono filament résorbable. La mobilisation du lambeau proximal muqueux représente le dernier temps opératoire. Celui-ci est abaissé ensuite au-delà de la suture musculaire, telle une persienne protégeant une fenêtre sans chevauchement direct des zones suturées (Fig. 9).
La plaie de l’ orifice secondaire est laissée ouverte afin d’ en assurer le drainage et recouverte d’ une mèche grasse pour 24 à 48 heures (28).
En phase postopératoire, on doit éviter toute constipation, ou diarrhée délétère pour le lambeau abaissé. Les douches pluriquotidiennes, six fois minimum de la plaie cutanée secondaire sont de rigueur. Un contrôle médical hebdomadaire jusqu’ à guérison complète par l’ opérateur, sans examen endo-anal jusqu’ à la 3ème semaine est recommandé. Le taux de récidive de ces fistules en fistules complexes dans notre expérience est de 25 % (29). Chez les patients fumeurs, ce taux peut doubler. Le tabagisme est donc un facteur important à la récidive des fistules anales après traitement chirurgical. Une des grandes questions est que faire en cas de récidive ?
Le lambeau d’avancement rectal (LAR) est une solution thérapeutique reconnue pour traiter des fistules anales complexes. Peu de données existent sur les résultats d’un nouveau lambeau d’avancement sur une fistule récidivante déjà opérée par cette procédure. Nous avons réalisé une étude afin d’évaluer les résultats d’un second lambeau d’avancement comme traitement de la fistule anale complexe récidivante après un premier lambeau.
Cette étude rétrospective, mono centrique porte sur 120 patients opérés par LAR d’une fistule anale crypto-glandulaire. 38 patients ont présenté une récidive de fistule (31,6 %). La récidive était complexe chez 29 patients (24.1 %) et simple chez 9 (7.5 %). Un second LAR a été réalisé chez les 29 ayant une récidive complexe. 83 % (24) de ces patients ont fermé leur fistule, alors que 17 % (5) ont présenté une seconde récidive.
Le LAR est une option intéressante pour la prise en charge d’une récidive de fistule anale complexe. Un premier lambeau n’altère pas les chances de guérison et n’augmente pas la morbidité. Un effet « down-staging », avec en particulier 24 % de fistules simples après un premier LAR, et une transformation des fistules complexes hautes (supra-sphinctériennes ou trans-sphinctériennes hautes) en basses de 16 %, permettent une prise en charge plus aisée de ces récidives (30).
Nouveautés thérapeutiques des fistules anales
LIFT (Ligation inter-sphincterial of fistula tract)
Cette technique LIFT, décrite en 2007 par Rojanasakul (31), a gagné en popularité en raison de sa facilité d’ exécution et de la préservation de la continence. Cette technique consiste à déconnecter l’ orifice primaire de la fistule du trajet au travers de l’ espace inter- sphinctérien en réséquant la zone de la glande infectée. Le taux de succès varie de 40 à 90 %. Les récidives semblent dues au résidu fistuleux laissé en place. Cette technique garanti un succès de 50 % et aucune lésion du sphincter avec seulement 5.5 % de complications post opératoires (32). Contrairement au LAR, le nombre de récidive augmente avec les réinterventions par LIFT (33).
Le grand avantage du LIFT, par rapport à toutes ces nouvelles techniques, est son coût limité.
VAAFT (Video Assisted Anal Fistula Treatment)
Le trajet de la fistule est visionné par un endoscope pédiatrique. Il est rincé, cureté puis, soit brûlé, soit rempli de colle de fibrine. L’ orifice interne est fermé par des fils ou une agrafeuse, ce qui augmente drastiquement le coût. Le taux de guérison se situe entre 58 et 87 % (34, 35).
Techniques d’ occlusion endo luminales
Injection de fibrine et de collagène
L’ utilisation de la colle de fibrine dans le traitement des fistules a été proposée en 1982 (36). Les premiers résultats étaient encourageants. La technique consiste à repérer le trajet fistuleux, le laver, le cureter. L’ encollage se fait ensuite à l’ aide de colle de fibrine, de collagène de colle biologique (37) ou synthétique par canulation du trajet de la fistule. La colle de fibrine, outre son effet occlusif, stimulerait selon les auteurs la cicatrisation du trajet fistuleux. Une étude prospective de Buchana (38) démontre un taux de succès de 14 %, 14 mois après le traitement. Nous avons appliqué la technique de l’ encollage en cas de fistules complexes comme les fistules urétro-rectales ou les fistules de Crohn. Dans ces conditions le taux de récidive est de 60 %, comparable à celui de la chirurgie avec l’ avantage d’ être moins délétère (16).
Injection de cellules germinales autologues
Les cellules mésenchymateuses adultes ont la capacité de se différencier. On peut les utiliser dans la régénération des tissus endommagés et donc dans les fistules. Quelques études toutes issues d’ Espagne prélèvent ces cellules par lipoaspiration du tissu adipeux. Après curetage de la fistule elles sont injectées dans le trajet et l’ orifice primaire est suturé.
Si les résultats sont médiocres (35 % de succès) pour les fistules crypto glandulaires, ils semblent encourageants pour les fistules de Crohn (39, 40). Le facteur limitant reste le coût important de ces techniques.
Plug anal
Le plug anal est un composé lyophilisé issu de tissu porcin dénué de cellules. Ce tissu est placé dans le trajet de la fistule après avoir nettoyé et débridé cette dernière en le tractant à l’ aide d’ un fil. Son extrémité proximale de diamètre supérieur est nouée au sphincter par un nœud en 8. L’ extrémité distale plus fine est sectionnée au niveau de la peau à l’ orifice externe. Les résultats encourageants des premières études n’ ont malheureusement pas pu être reproduits, le taux de succès est de 24 % dans une étude randomisée comparant plug et LAR (29). Notre expérience reflète parfaitement ces résultats puisque nous avons placés 20 plugs avec 1 seul succès.
Laser
L’ application de laser endoluminal a pour but de détruire l’ épithélium résiduel responsable d’ une partie des récidives. Ce laser devrait permettre une oblitération thermique de la fistule Le succès initial reporté chez 11 patient est de 81 % avec un suivi court de
7 mois (41). Une étude menée sur 35 patients porteurs de fistules de Crohn montre une guérison dans 71 % des cas ce qui est très surprenant (42). Le guideline allemand sur les abcès et fistules conclut d’ ailleurs au sujet de ce traitement : Aucune recommandation ne peut être donnée en raison des résultats actuels (15).
A ce jour, il est difficile de se faire une opinion objective sur ces nouvelles techniques. Beaucoup de questions restent sans réponse incluant le bien fondé et surtout les conflits d’ intérêts évidents que génèrent les coûts liés à ces traitements (43).
De toutes ces nouvelles techniques la seule qui échappe à ce raisonnement est le LIFT.
Conclusions
La pathologie abcédée de la région ano-rectale est extrêmement fréquente et doit être prise en charge sans délai. Son traitement consiste en un drainage chirurgical en urgence sous éventuelle couverture antibiotique. Il peut être réalisé dans la majorité des cas sous anesthésie locale.
Lorsque la phase aiguë est passée, le ou les trajets fistuleux sont recherchés. La mise en place d’ un fil de séton permet le drainage et génère la sclérose des fistules.
Après exclusion d’ une maladie sous-jacente ou fistulisante, il est procédé au traitement chirurgical de la fistule. La technique est adaptée à la quantité de muscle sphincter mise en danger par l’ incision chirurgicale. De nombreuses techniques existent pour le traitement des fistules, ce qui démontre la complexité de cette maladie et la non reproductibilité des résultats de ces traitements.
Dans ces conditions, les techniques classiques gardent toute leur valeur. Le LAR reste l’ intervention de référence pour traiter les fistules complexes. Le LIFT de par sa simplicité, son coût limité et ses résultats encourageants pourrait jouer un rôle important dans le futur du traitement des fistules. Les techniques d’ occlusions sont séduisantes mais pour l’ instant les résultats sont insuffisants, surtout si on considère le rapport coût qualité.
Pour toutes ces raisons, il reste important d’ adapter la technique chirurgicale au type de fistule à traiter et non la fistule à la technique chirurgicale.
Dr Karel Skala Pr Roland Chautems Dr Guillaume Zufferey
Pr Bruno Roche
Centre de proctopérinéologie Clinique des Grangettes
chemin des Grangettes 7
1224 Chêne-Bougeries
bruno.roche@grangettes.ch
Les auteurs n’ont déclaré aucun conflit d’intérêts en relation avec cet article.
La plupart des abcès para-anaux sont primaires et proviennent de l’ infection d’ une glande inter-sphinctérienne. L’ abcès situé à l’ origine dans l’ espace inter-sphinctérien se draine en suivant les voies de moindre résistance et constitue ainsi un abcès para-anal, ischio-rectal, en fer à cheval, pelvi-rectal ou inter-sphinctérien. Le diagnostic est plutôt aisé dans les présentations classiques d’ abcès para-anal. Il devient plus difficile lors d’ abcès inter-sphinctérien ou de la fosse ischio-rectale. Le diagnostic peut être précisé par un examen endoscopique, une échographie endo-anale ou IRM du pelvis.
La pierre angulaire du traitement de l’ abcès ano-rectal est le drainage chirurgical. Il peut être assuré par le praticien formé. Celui-ci peut le réaliser souvent en anesthésie locale, sans couverture antibiotique et les cultures de germes ne s’ imposent pas.
Le traitement chirurgical est une urgence et ce geste ne doit pas être repoussé. Cette attitude est motivée par le spectre dramatique d’ une évolution vers un sepsis sévère ou une gangrène de Fournier. L’ orifice fistulaire primaire endoanal n’ est pas recherché à la phase aiguë.
25% des cas ferment définitivement et spontanément leur trajet fistuleux. Dans les autres cas de figure, on place un drainage préopératoire en séton et l’ option thérapeutique chirurgicale est choisie en fonction de la localisation et de la complexité de la maladie fistulaire.
1. Sainio P. Fistula-in-ano in a defined population. Incidence and epidemiological aspects. Annales chirurgiae et gynaecologiae. 1984;73(4):219-24.
2. Ramanujam PS, Prasad ML, Abcarian H, Tan AB. Perianal abscesses and fistulas. A study of 1023 patients. Diseases of the colon and rectum. 1984;27(9): 593-7.
3. Klosterhalfen B, Offner F, Vogel P, Kirkpatrick CJ. Anatomic nature and surgical significance of anal sinus and anal intramuscular glands. Diseases of the colon and rectum. 1991;34(2):156-60.
4. Zanotti C, Martinez-Puente C, Pascual I, Pascual M, Herreros D, Garcia-Olmo D. An assessment of the incidence of fistula-in-ano in four countries of the European Union. International journal of colorectal disease. 2007;22(12):1459-62.
5. Adamo K, Sandblom G, Brannstrom F, Strigard K. Prevalence and recurrence rate of perianal abscess–a population-based study, Sweden 1997-2009. International journal of colorectal disease. 2016;31(3):669-73.
6. Devaraj B, Khabassi S, Cosman BC. Recent smoking is a risk factor for anal abscess and fistula. Diseases of the colon and rectum. 2011;54(6):681-5.
7. Wang D, Yang G, Qiu J, Song Y, Wang L, Gao J, et al. Risk factors for anal fistula: a case-control study. Techniques in coloproctology. 2014;18(7):635-9.
8. Cioli VM, Gagliardi G, Pescatori M. Psychological stress in patients with anal
fistula. International journal of colorectal disease. 2015;30(8):1123-9.
9. Hamilton CH. Anorectal problems: the deep postanal space–surgical significance in horseshoe fistula and abscess. Diseases of the colon and rectum. 1975;18(8):642-5.
10. Bussen D, Sailer M, Wening S, Fuchs KH, Thiede A. [Usefulness of anal endosonography in the assessment of fistula-in-ano]. Zentralblatt fur Chirurgie. 2004;129(5):404-7.
11. Badrinath K, Jairam N, Ravi HR. Spreading extraperitoneal cellulitis following perirectal sepsis. The British journal of surgery. 1994;81(2):297-8.
12. Yilmazlar T, Ozturk E, Ozguc H, Ercan I, Vuruskan H, Oktay B. Fournier’s gangrene: an analysis of 80 patients and a novel scoring system. Techniques in coloproctology. 2010;14(3):217-23.
13. Di Falco G, Guccione C, D’Annibale A, Ronsisvalle S, Lavezzo P, Fregonese D, et al. Fournier’s gangrene following a perianal abscess. Diseases of the colon and rectum. 1986;29(9):582-5.
14. Ozturk E, Sonmez Y, Yilmazlar T. What are the indications for a stoma in Fournier’s gangrene? Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. 2011;13(9):1044-7.
15. Ommer A, Herold A, Berg E, Furst A, Post S, Ruppert R, et al. German S3 guidelines: anal abscess and fistula (second revised version). Langenbeck’s archives of surgery. 2017;402(2):191-201.
16. Hamalainen KP, Sainio AP. Incidence of fistulas after drainage of acute anorectal abscesses. Diseases of the colon and rectum. 1998;41(11):1357-61; discussion 61-2.
17. Rizzo JA, Naig AL, Johnson EK. Anorectal abscess and fistula-in-ano: evidence-based management. The Surgical clinics of North America. 2010;90(1):45-68, Table of Contents.
18. Cheong DM, Nogueras JJ, Wexner SD, Jagelman DG. Anal endosonography for recurrent anal fistulas: image enhancement with hydrogen peroxide. Diseases of the colon and rectum. 1993;36(12):1158-60.
19. Kolodziejczak M, Santoro GA, Obcowska A, Lorenc Z, Manczak M, Sudol-Szopinska I. Three-dimensional endoanal ultrasound is accurate and reproducible in determining type and height of anal fistulas. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. 2017;19(4):378-84.
20. Siddiqui MR, Ashrafian H, Tozer P, Daulatzai N, Burling D, Hart A, et al. A diagnostic accuracy meta-analysis of endoanal ultrasound and MRI for perianal fistula assessment. Diseases of the colon and rectum. 2012;55(5):576-85.
21. Parks AG, Gordon PH, Hardcastle JD. A classification of fistula-in-ano. The British journal of surgery. 1976;63(1):1-12.
22. McCourtney JS, Finlay IG. Setons in the surgical management of fistula in ano. The British journal of surgery. 1995;82(4):448-52.
23. Ritchie RD, Sackier JM, Hodde JP. Incontinence rates after cutting seton treatment for anal fistula. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. 2009;11(6):564-71.
24. Vial M, Pares D, Pera M, Grande L. Faecal incontinence after seton treatment for anal fistulae with and without surgical division of internal anal sphincter: a systematic review. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. 2010;12(3):172-8.
25. Gottgens KW, Janssen PT, Heemskerk J, van Dielen FM, Konsten JL, Lettinga T, et al. Long-term outcome of low perianal fistulas treated by fistulotomy: a multicenter study. International journal of colorectal disease. 2015;30(2):213-9.
26. van Tets WF, Kuijpers HC. Continence disorders after anal fistulotomy. Diseases of the colon and rectum. 1994;37(12):1194-7.
27. Ratto C, Litta F, Donisi L, Parello A. Fistulotomy or fistulectomy and primary sphincteroplasty for anal fistula (FIPS): a systematic review. Techniques in coloproctology. 2015;19(7):391-400.
28. Ozuner G, Hull TL, Cartmill J, Fazio VW. Long-term analysis of the use of transanal rectal advancement flaps for complicated anorectal/vaginal fistulas. Diseases of the colon and rectum. 1996;39(1):10-4.
29. Ortiz H, Marzo J, Ciga MA, Oteiza F, Armendariz P, de Miguel M. Randomized clinical trial of anal fistula plug versus endorectal advancement flap for the treatment of high cryptoglandular fistula in ano. The British journal of surgery. 2009;96(6):608-12.
30. Podetta M, Scarpa CR, Zufferey G, Skala K, Ris F, Roche B, et al. Mucosal advancement flap for recurrent complex anal fistula: a repeatable procedure. International journal of colorectal disease. 2019;34(1):197-200.
31. Rojanasakul A, Pattanaarun J, Sahakitrungruang C, Tantiphlachiva K. Total anal sphincter saving technique for fistula-in-ano; the ligation of intersphincteric fistula tract. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2007;90(3):581-6.
32. Sirany AM, Nygaard RM, Morken JJ. The ligation of the intersphincteric fistula tract procedure for anal fistula: a mixed bag of results. Diseases of the colon and rectum. 2015;58(6):604-12.
33. Abcarian AM, Estrada JJ, Park J, Corning C, Chaudhry V, Cintron J, et al. Ligation of intersphincteric fistula tract: early results of a pilot study. Diseases of the colon and rectum. 2012;55(7):778-82.
34. Kochhar G, Saha S, Andley M, Kumar A, Saurabh G, Pusuluri R, et al. Video-
assisted anal fistula treatment. JSLS : Journal of the Society of Laparoendoscopic Surgeons. 2014;18(3).
35. Meinero P, Mori L. Video-assisted anal fistula treatment (VAAFT): a novel sphincter-saving procedure for treating complex anal fistulas. Techniques in coloproctology. 2011;15(4):417-22.
36. Hedelin H, Nilson AE, Teger-Nilsson AC, Thorsen G. Fibrin occlusion of fistulas postoperatively. Surgery, gynecology & obstetrics. 1982;154(3):366-8.
37. Giordano P, Sileri P, Buntzen S, Stuto A, Nunoo-Mensah J, Lenisa L, et al. A prospective multicentre observational study of Permacol collagen paste for anorectal fistula: preliminary results. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. 2016;18(3):286-94.
38. Buchanan GN, Bartram CI, Phillips RK, Gould SW, Halligan S, Rockall TA, et al. Efficacy of fibrin sealant in the management of complex anal fistula: a prospective trial. Diseases of the colon and rectum. 2003;46(9):1167-74.
39. Garcia-Olmo D, Herreros D, Pascual I, Pascual JA, Del-Valle E, Zorrilla J, et al. Expanded adipose-derived stem cells for the treatment of complex perianal fistula: a phase II clinical trial. Diseases of the colon and rectum. 2009;52(1):79-86.
40. Herreros MD, Garcia-Arranz M, Guadalajara H, De-La-Quintana P, Garcia-Olmo D, Group FC. Autologous expanded adipose-derived stem cells for the treatment of complex cryptoglandular perianal fistulas: a phase III randomized clinical trial (FATT 1: fistula Advanced Therapy Trial 1) and long-term evaluation. Diseases of the colon and rectum. 2012;55(7):762-72.
41. Wilhelm A. A new technique for sphincter-preserving anal fistula repair using a novel radial emitting laser probe. Techniques in coloproctology. 2011;15(4): 445-9.
42. Giamundo P, Geraci M, Tibaldi L, Valente M. Closure of fistula-in-ano with laser–FiLaC: an effective novel sphincter-saving procedure for complex disease. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. 2014;16(2):110-5.
43. Limura E, Giordano P. Modern management of anal fistula. World journal of gastroenterology. 2015;21(1):12-20.
Un dentiste retraité de 72 ans souffre de diabète sucré de type 2 depuis au moins 15 ans dans le cadre d’ un syndrome métabolique. Lors de l’ examen, vous constatez une insuffisance rénale progressive. Quelles sont les considérations thérapeutiques appropriées ? Cet article présente des suggestions bien fondées.
L’ homme de 72 ans atteint de diabète sucré de type 2 de longue date a bénéficié pendant de nombreuses années d’ un bon contrôle glycémique avec la metformine et Jardiance® 10 mg par jour pendant environ 2 ans. Il a bien répondu aux deux médicaments et a atteint des valeurs d’ HbA1c de 6,5-7 %. Le patient se réjouit de recevoir la plus moderne et meilleure thérapie existante. Il
vient dans votre cabinet de médecin généraliste pour en discuter. Il s’ est acheté un glucomètre capillaire et mesure de temps en temps sa glycémie à jeun, le plus souvent autour de 8 mmol / l avec des valeurs préprandiales d’ environ 8-10 mmol / l.
Anamnèse personnelle
lDiabète sucré de type 2, diagnostiqué pour la première fois il y a 15 ans avec les lésions secondaires des organes suivantes : coronaropathie coronarienne stable et AOMI de stade IIa, polyneuropathie périphérique, insuffisance rénale chronique avec microalbuminurie.
lCardiopathie coronarienne, premier diagnostic il y a 5 ans avec une fraction d’ éjection ventriculaire gauche d’ environ 45 %.
Taille 168 cm, 78 kg, IMC 27,6 kg / m2, tension artérielle 144 / 75, pouls 64 / min, réflexes rotulien et achilléen non déclenchables, monofilament 10 / 10 des deux côtés, sens de vibration 4 / 8 des deux côtés.
Laboratoire
HbA1c 7,6 %,
eGFR selon CKD-EPI 28 ml / min (il y a 2 ans : 45 ml / min)
LDL 2,5 mmol / l
Hémoglobine 105 g / l
Vitamine B12 175 ng / l (norme > 190 ng / l)
Ferritin 64 μg / l (norme 30 – 400 μg / l
CRP 1,5 mg / l (norme < 5 mg / l)
La thérapie doit-elle être laissée telle quelle ?
Si la fonction rénale est altérée (eGFR < 30 ml / min), il faut arrêter d’ administrer la metformine et l’ inhibiteur de SGLT-2. Bien que l’ effet hypoglycémiant des inhibiteurs de la SGLT-2 diminue avec la diminution de la fonction rénale, les propriétés rénoprotectrices et cardioprotectrices demeurent intactes, ce qui est particulièrement important avec une FEVG de 45 %. Dans les études portant sur les paramètres cardiovasculaires, l’ empagliflozine (Jardiance®) et, plus particulièrement la canagliflozine (Invokana®), ont démontré un bénéfice cardiovasculaire et rénal pouvant atteindre 30 ml/min eGFR.
C’ est pour ces raisons que le traitement par Jardiance pourrait être interrompu si la fonction rénale ne se détériore pas davantage. Toutefois, en cas de maladie aiguë, de chirurgie, etc., la Jardiance doit être arrêtée immédiatement (risque d’ acidocétose).
La metformine pourrait être remplacée par un inhibiteur de la DPP-4, Trajenta® (linagliptine) 5 mg. C’ est un traitement sûr pour abaisser la glycémie, mais il n’ a pas d’ effet positif sur les critères d’ évaluation rénovasculaires et cardiovasculaires.
Si l’ IMC était de ≥ 28 kg / m2, nous pourrions aussi envisager un traitement avec un agoniste des récepteurs GLP1, par exemple l’ Ozempic® hebdomadaire (semaglutide), qui peut être administré jusqu’ à un eGFR de 10 ml / min. Il a été démontré que les GLP1-RA ont un effet positif sur les paramètres cardiovasculaires et rénaux.
Une autre possibilité serait l’ insulinothérapie (insuline de base (par exemple Tresiba® ou Glargine 300 Toujeo®) ou Ryzodeg® co-formulé (70 % d’ insuline Tresiba et 30 % de NovoRapid)), ou une sulfonylurée à action rapide sans métabolites actifs (par exemple gliclazide 30-60 mg/jour). Les deux alternatives présentent un risque d’ hypoglycémie. Les insulines ultra-longues Tresiba® et Toujeo® présentant un risque d’ hypoglycémie considérablement plus faible que les insulines NPH, les insulines mixtes (Mixtard, Humalog® Mix) ou Lantus® et Levemir®.
Le diabète sucré de type 2 est-il bien ajusté avec une HbA1c de 7,6 % ?
Tout d’ abord, la crédibilité de la valeur de l’ HbA1c doit être remise en question, car divers facteurs affectant l’ érythropoïèse peuvent rendre la valeur de l’ HbA1c erronément élevée ou faible. Dans le cas d’ une carence en vitamine B12, les valeurs d’ HbA1c sont plutôt surestimées. Dans le cas d’ insuffisance rénale chronique, elles sont plutôt faussement faibles. Les valeurs de glycémie mesurées par voie capillaire donnent une moyenne d’ environ 9 mmol / l, ce qui correspond bien à l’ HbA1c de 7,6 % et démontre que l’ effet changeant de la carence en vitamine B12 et l’ insuffisance rénale s’ annulent approximativement.
Chez les patients de 72 ans atteints de divers dommages secondaires aux organes, l’ objectif thérapeutique principal est l’ absence d’ hypoglycémie et un taux d’ HbA1c acceptable de 7,6 % (taux cible d’ HbA1c 7,5 %). Si un traitement sans risque d’ hypoglycémie est utilisé, par exemple un inhibiteur de la SGLT-2, de la GLP-1 RA ou de la DPP-4, il faudrait que le patient ait une HbA1c aussi normale que possible (< 7,0 %).
La tension artérielle systolique est légèrement trop élevée. Cependant, il ne faudrait pas non plus que la pression artérielle diastolique soit inférieure à 70 mm Hg. La grande différence entre la tension artérielle systolique et diastolique peut probablement s’ expliquer par la médiasclérose typique. Éventuellement, la dose de l’ inhibiteur de l’ ECA et/ou de l’ antagoniste du calcium pourrait être légèrement augmentée.
Pr Roger Lehmann
Clinique d’endocrinologie, de diabétologie et nutrition clinique
Hôpital universitaire de Zurich
Rämistrasse 100
8091 Zurich
RL: Participation à des Advisory Boards et honoraires de conférencier avec Novo, Nordisk, Sanofi, MSD, Boehringer Ingelheim, Servier et Astra Zeneca.
ME: Frais de voyage et de congrès d’ Eli Lilly et Ipsen.
Traitement du diabète sucré de type 2 à eGFR < 30 ml / min
– Pas de metformine (danger d’ acidose lactate)
– Amélioration prouvée du risque cardiovasculaire et rénal :
– Inhibiteurs de SGLT2 jusqu’ à un eGFR de 30 ml/min avec effet cardioprotecteur et renoprotecteur prouvé (baisse de l’ hypoglycémie)
– Agonistes des récepteurs GLP1 (p. ex. Ozempic à eGFR 10 ml/min approuvé) si IMC ≥ 28 kg / m2.
Inhibiteurs de la DPP4 (p. ex. Trajenta 5 mg / jour) sûrs, mais sans effet bénéfique pour les paramètres cardiovasculaires et rénaux. Insuline ou sulfonylurées à action rapide sans métabolites actifs (p. ex. gliclazide)
« Sick day rules » : Arrêter la metformine et les inhibiteurs de la SGLT2 dans les cas de maladie aiguë, vomissements, diarrhée, chirurgie, etc.
Toujours remettre en question la valeur de l’ HbA1c et, en cas de doute ou de difficulté d’ interprétation dans des situations particulières, la comparer avec les mesures de glycémie capillaire.
– Principales causes de fausses valeurs élevées d’ HbA1c : anémie ferriprive et carence en vitamine B12.
– Principales causes de fausses valeurs faibles d’ HbA1c : insuffisance rénale chronique, néosynthèse d’ érythrocytes (par ex. carence en fer fraîchement supplémentée), anémie hémolytique et cirrhose du foie.
La pneumonie acquise en communauté est définie comme étant une pneumonie survenant à l’ extérieur de l’ hôpital chez un patient qui n’ est pas immunodéprimé. Il ne faut pas sous-estimer le taux de létalité allant jusqu’ à 10 % chez les patients hospitalisés en raison d’ une progression grave. Pour de nombreuses personnes âgées malades, la polymorbidité est un facteur de complication. Si, et tant qu’ un objectif thérapeutique curatif existe, la sévérité et le spectre bactérien attendu ainsi que la présence ou non d’ une polymorbidité détermine la thérapie à suivre.
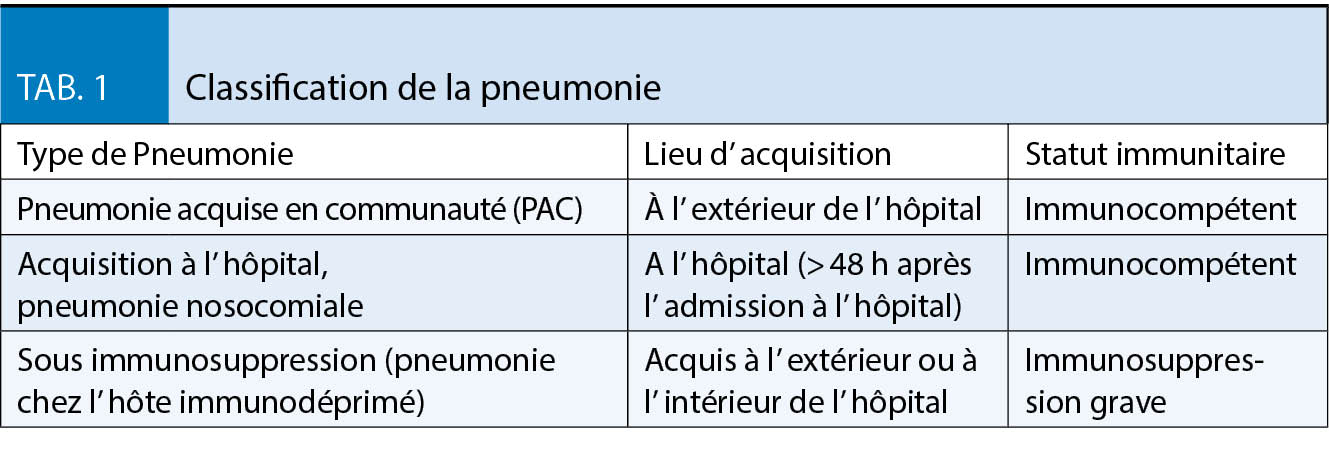
La pneumonie est classée selon les critères du tableau 1. La pneumonie acquise en communauté (PAC) est définie comme une pneumonie déterminée par le lieu de survenue (en dehors de l’ hôpital) et l’ immunité du patient (compétence immunitaire). Elle contraste avec la pneumonie nosocomiale, qui est définie comme une pneumonie qui survient > 48 heures après l’ admission à l’ hôpital ou chez les patients ayant déjà été hospitalisés au maximum il y a trois mois. En cas de pneumonie chez l’ immunodéprimé sévère, des germes opportunistes sont à prévoir.
Les patients polymorbides sont des patients atteints de maladies pulmonaires chroniques comme la BPCO, la mucoviscidose et les maladies pulmonaires interstitielles ainsi que le diabète sucré, une hépatopathie et les maladies tumorales sans neutropénie (1).
L’ incidence de la PAC augmente avec l’ âge. La pneumonie chez les personnes âgées (≥ 65 ans) est associée à une mortalité accrue. La pneumonie contractée dans les EMS représente le sous-groupe le plus important de la PAC. La létalité la plus élevée se produit chez les patients alités depuis un certain temps.
La PAC des personnes de moins de 65 ans, sans maladie sous-jacente est généralement plus légère et le pronostic est nettement meilleur. Elles sont en général dues à d’ autres types de germes pathogènes.
Classification de PAC
La PAC est divisée en groupes (1a, 1b et 2) qui définissent les critères d’ hospitalisation ainsi que la portée du diagnostic microbiologique et les stratégies thérapeutiques, y compris la thérapie antimicrobienne initiale. Les groupes 1a, 1b et 2 se distinguent par les critères de l’ état de santé général et de la gravité de la PAC. L’ appartenance au groupe 1a résulte d’ un bon état de santé général, défini comme un repos au lit < 50 % de la journée. Le groupe 1b à un mauvais état général, défini comme un repos au lit > 50 % de la journée. L’ appartenance au groupe 2 résulte d’ une comorbidité sévère avec un pronostic défavorable. Souvent, la palliation est l’ objectif thérapeutique prédominant dans ce dernier groupe. Les formes particulières de PAC sont la pneumonie d’ aspiration acquise en communauté, celle contractée dans le cadre d’ un voyage à l’ étranger, causée par une épidémie (p. ex. pneumonie grippale) ou par un foyer (p. ex. Legionella). La pneumonie par aspiration est associée à une modification du spectre pathogène. Elle nécessite une clarification des causes sous-jacentes. Dans le cas d’ une pneumonie à la suite d’ un voyage tropical, les causes rares doivent être recherchées et écartées. En période d’ épidémie de grippe, il faut aussi penser à la pneumonie grippale.
Diagnostic d’ une pneumonie suspectée
Les symptômes cliniques de la pneumonie comprennent :
1. symptômes respiratoires tels que la toux avec ou sans expectorations, dyspnée, et éventuellement douleurs thoraciques respiratoires.
2. symptômes généraux tels que la fièvre ou hypothermie, sensation générale de maladie («malaise»), symptômes «grippaux» tels que myalgie, arthralgie, céphalées, palpitations, troubles circulatoires, diarrhées.
3. symptômes neurologiques, en général un état confusionnel aigu qui est la forme de présentation la plus fréquente chez les résidents de long séjour comme par exemple un changement brutal de l’ état cognitif, des troubles attentionnels ou une désorientation. L’ examen clinique comprend l’ évaluation de l’ état général, y compris l’ état fonctionnel (indépendance dans les activités de la vie quotidienne) et la mobilité, en particulier l’ importance d’ un éventuel alitement préexistant qui indique un moins bon pronostic. Il comprend en outre une évaluation des comorbidités potentiellement instables (pronostic moins bon). Puis, les résultats suivants sont examinés en détail : augmentation de la fréquence respiratoire, tachycardie, hypotension artérielle possible, matité à la percussion lors de foyers consolidés et/ou d’ épanchement pleural parapneumonique, râles crépitants fins auscultatoire et souffle tubaire dans les cas de bronchopneumonie lobaire. Ces symptômes ne sont pas spécifiques pour distinguer une PAC d’ autres infections des voies respiratoires inférieures. Toutefois, l’ examen clinique a une valeur prédictive négative élevée (4). Avec l’ âge, les patients atteints de pneumonie deviennent de plus en plus oligosymptomatiques (5). Ainsi, la présence de fièvre ou de toux avec expectorations est significativement plus rare. Plus fréquemment, des symptômes tels qu’ un état confusionnel ou des diarrhées (bronchopneumonie de la base) peuvent être les seuls signes présents. Une radiographie du thorax doit être faite lors d’ examens complémentaires. L’ échographie thoracique peut être utilisée pour la détection des infiltrations pulmonaires lorsque la radiologie n’ est pas disponible en temps opportun. Les résultats radiologiques servent à déterminer l’ étendue des pathologies ainsi que les maladies concomitantes (ex. insuffisance cardiaque) et les complications (épanchement pleural, abcès). En outre, l’ examen radiologique fournit une aide pour le diagnostic différentiel (tuberculose pulmonaire, carcinome bronchique) ainsi qu’ une première indication pour déterminer si un contrôle est indiqué dans l’ évolution de la maladie. Cependant, la sensibilité, la spécificité ainsi que la fiabilité de la détection d’ un infiltrat dans l’ image radiographique du thorax sont limitées.
Des infiltrats se forment parfois au cours de la maladie. Dans une étude, 21 % des patients qui ont été diagnostiqués avec une pneumonie n’ avaient aucun infiltrat radiologique initialement (6). De plus, dans le cas d’ une pneumonie légère à modérée, l’ évaluation des infiltrats dépend considérablement de l’ investigateur concerné. En effet, la mortalité augmente chez les patients hospitalisés atteints d’ une pneumonie confirmée qui n’ avaient initialement pas de corrélation radiologique. Les paramètres d’ inflammation peuvent aider dans cette situation. Le CRP en tant que paramètre unique n’ est pas spécifique et peut augmenter avec un retard. La procalcitonine (PCT) est un biomarqueur sérique qui augmente en réponse aux infections bactériennes. Étant donné que l’ exactitude diagnostique de la procalcitonine est seulement modérée, elle n’ est pas utilisée de façon systématique pour faciliter le diagnostic de la PAC. Cependant, il est recommandé d’ obtenir un taux de procalcitonine au moment du diagnostic de PAC, et en série par la suite, pour aider à déterminer la durée appropriée des antibiotiques. Mesure de la saturation en O2 périphérique, analyse éventuelle des gaz du sang artériel (hypoxémie indique un mauvais pronostic).
Examen microbiologique d’ un patient atteint de pneumonie ?
Un diagnostic microbiologique n’ est normalement pas nécessaire pour les patients atteints d’ une pneumonie légère. En effet, ils peuvent être traités en ambulatoire.
Tous les patients des groupes 1a et 1b hospitalisés pour une pneumonie modérée à grave doivent recevoir un diagnostic de l’ agent pathogène. Il s’ agit notamment de :
1. au moins deux hémocultures, aérobie et anaérobie, respectivement.
2. test d’ antigène urinaire pour les légionelles.
3. test d’ antigène urinaire pour pneumocoques pour la détection de la pneumonie par pneumocoques.
4. l’ expectoration adéquate doit être traitée dans les 2 à 4 heures pour la coloration de Gram ainsi que pour la culture. Si cela est impossible, un examen des expectorations ne devrait pas être fait.
5. le diagnostic moléculaire pour la détection simultanée de plusieurs bactéries (par exemple S. pneumoniae, M. pneumoniae,
C. pneumoniae, L. pneumophila) ou agents pathogènes viraux (par exemple influenza A/B, parainfluenza, rhinovirus, adénovirus), c’est-à-dire les tests dits multiplex ne devraient pas être utilisés systématiquement.
6. une recherche sur frottis nasal par amplification de l’ acide nucléaire pour la grippe A/B doit être effectuée s’ il y a des indices d’ une épidémie de grippe (saison, épidémie et pandémie).
Dans l’ ensemble, les hémocultures ne sont positives que chez environ 10 % des patients hospitalisés pour une PAC. Dans le cas d’ une pneumonie à pneumocoques, ces taux sont un peu plus élevés, selon diverses études, dans une fourchette de 27 à 38 % (15, 16). En outre, la pneumonie bactérienne peut être associée à un pronostic plus défavorable, de sorte qu’ une hémoculture positive peut être une raison pour intensifier la surveillance. L’ hémoculture est également plus fréquemment positive chez les patients âgés et dans les cas de pneumonie causée par des entérobactéries. En outre, la détection des agents pathogènes dans les hémocultures constitue la preuve étiologique la plus sûre.
Le test d’ antigène urinaire pour Legionella détecte l’ infection à Legionella par Legionella pneumophila des sérogroupes communs avec une sensibilité d’ environ 75 % et une spécificité de 99-100 %. Si d’ autres espèces ou sérogroupes sont également attendus en raison de la situation épidémiologique, un test d’ amplification de l’ acide nucléique à partir de matériel respiratoire doit être effectué et des preuves culturelles doivent être fournies.
Le test d’ antigène urinaire pour les pneumocoques détecte une infection par ces micro-organismes avec une sensibilité de 67-82% et une spécificité d’ environ 97 %. Les facteurs de risque pour un résultat faussement positif (en particulier la BPCO) doivent cependant être considérés. Le test peut donc servir de base à la focalisation de la thérapie.
Bien que la valeur de l’ examen microscopique et la culture des expectorations aient été plus souvent évaluées de façon critique, d’ autres études montrent que, si tous les critères de qualité (prédominance de granulocytes, peu ou pas d’ épithéliums pavimenteux) sont respectés, les résultats de l’ examen peuvent servir de guide pour la thérapie ciblée. En effet, Streptococcus pneumoniae, Haemophilus influenzae et Staphylococcus aureus sont notamment bien identifiés.
Diagnostic différentiel de la pneumonie
Chez tous les patients atteints d’ une PAC, un diagnostic différentiel ou additionnel doit être envisagé. Particulièrement en cas de surhydratation (maladie rénale), d’ aspiration et d’ infiltrats non infectieux (embolie pulmonaire, maladie pulmonaire interstitielle, cancer du poumon) ainsi que de BPCO et d’ emphysème pulmonaire.
La présentation clinique non spécifique, avec souvent aussi des patients oligosymptomatiques, rendent nécessaire d’ établir une distinction diagnostique différentielle avec d’ autres maladies dont les symptômes se chevauchent.
Estimation de la sévérité de la PAC
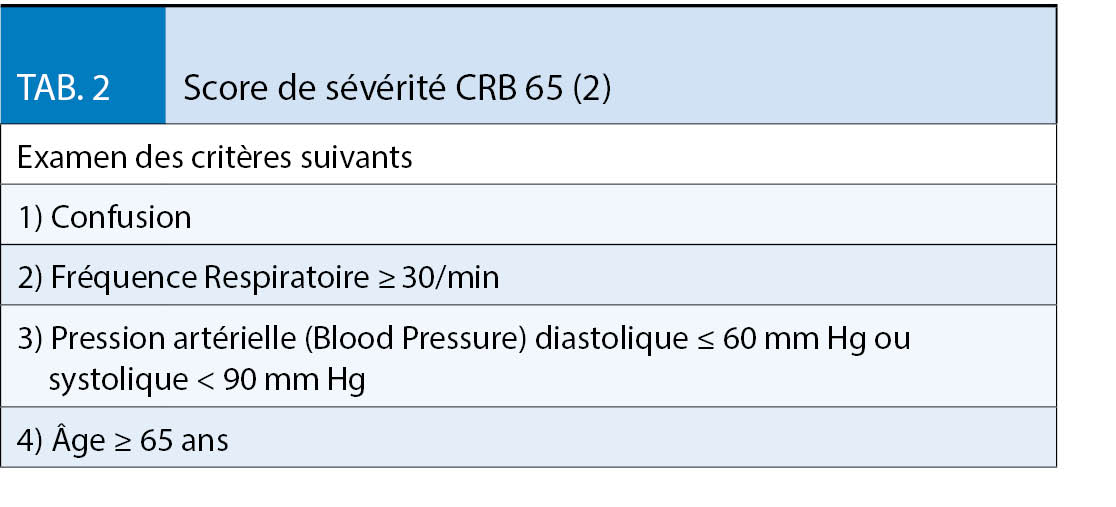
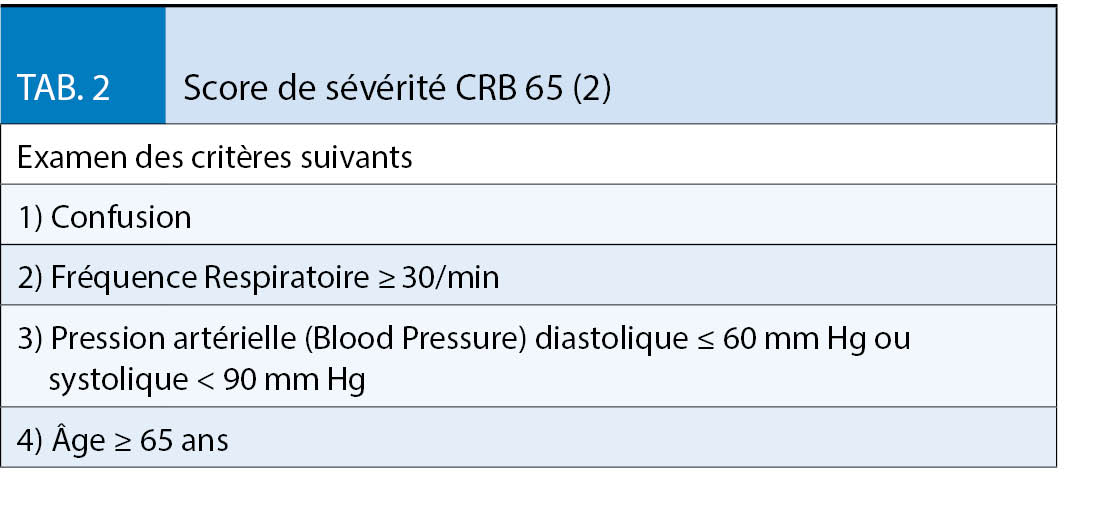
L’ indice CRB 65 (tabl. 2) s’ est imposé comme un score simple ayant une bonne prédiction du risque de létalité. Avec un score de 0, la létalité est de 0%, avec 1 : 3,3 %, avec 2 : 10% et avec 3 / 4 : 20,3 % (2). Il est formé par la détermination de trois simples paramètres cliniques et d’ un paramètre anamnestique. Il peut également être facilement appliqué sur une base ambulatoire. Le score est calculé en ajoutant un point pour chacun des critères énumérés au tabl. 2. A partir d’ un score de 1, une hospitalisation doit être envisagée. L’indice CRB-65 a été validé dans de nombreuses études et plusieurs méta-analyses actuelles.
Traitement de la PAC
Traitement antimicrobien initial
Les patients de moins de 65 ans atteints de pneumonie légère sans comorbidité devraient recevoir une monothérapie avec un macrolide (azithromycine, clarithromycine) comme traitement initial de choix.
Les patients atteints de pneumonie légère et de comorbidités définies doivent recevoir un traitement initial par un aminopénicilline / β-lactamine. Alternativement, une fluoroquinolone (Moxifloxacine, Lévofloxacine) peut être utilisée pour les allergies ou intolérances à la pénicilline. Dans les cas graves de BPCO et/ou de bronchectasie, un traitement par l’ amoxicilline/ciprofloxacine ou la lévofloxacine peut être administré.
Les patients atteints d’ une pneumonie modérée devraient recevoir comme traitement antimicrobien initial une aminopénicilline ou une céphalosporine de classe 2 ou 3a (cefpodoxime, céfuroxime) ainsi qu’ un macrolide. Si aucun agent pathogène bactérien atypique n’ est détecté pendant la stabilisation clinique, le traitement aux macrolides doit être interrompu après 3 jours. Par ailleurs, les patients atteints d’une PAC peuvent être traités avec une fluoroquinolone (moxifloxacine, lévofloxacine).
Chez les patients hospitalisés atteints d’ une pneumonie modérée, un traitement antimicrobien doit être administré par voie parentérale au cours des premiers jours. Les patients atteints d’ une pneumonie grave doivent d’ abord recevoir une thérapie combinée intraveineuse à large spectre à base de ß-lactamine (pipéracilline/tazobactam, céfotaxime ou ceftriaxone) ainsi qu’ un macrolide. En cas de stabilisation clinique et de détection manquante d’ un agent pathogène bactérien atypique, le traitement aux macrolides doit être interrompu après 3 jours. La monothérapie avec une fluoroquinolone (Moxifloxacine, Lévofloxacine) est une alternative possible, mais uniquement pour les patients sans choc septique.
En cas de pandémie de grippe ou d’ activité grippale saisonnière élevée, l’ oseltamivir (inhibiteur de la neuraminidase) peut être administrée précocement en plus du traitement antibactérien surtout chez les patients hospitalisés atteints de pneumonie modérée ou grave. Si la détection par PCR de l’ influenza demeure négative, il faut interrompre le traitement d’ oseltamivir.
Thérapie contrôlée par des biomarqueurs
L’ indication d’ un traitement et le contrôle de sa durée à l’ aide du biomarqueurs procalcitonine (PCT) a fait l’ objet de plusieurs études, en particulier d’ une étude Cochrane. Une condition préalable à une telle stratégie est que le PCT soit déterminé séquentiellement dans le cadre d’ un protocole. De plus, des recommandations d’ arrêt non ambiguës doivent être définies en fonction de seuils prédéterminés. Dans toutes les études, le clinicien était également ouvert à une «abrogation», c’ est-à-dire l’ abrogation des recommandations d’ arrêt en fonction de son jugement clinique.
Toutes les études ont montré que le traitement antimicrobien guidé par PCT permettait de raccourcir la durée du traitement (13), tant chez les patients hospitalisés que chez les patients en soins intensifs, sans et avec septicémie grave. Il n’ y avait aucune différence en ce qui concerne l’ échec du traitement ou la mortalité. Ce résultat a été confirmé dans une méta-analyse, particulièrement chez les patients atteints de PAC (13, 14).
Examens de suivi
Laboratoire
La détermination d’ un paramètre inflammatoire (CRP ou PCT) doit être effectuée dans le sérum à l’ admission ainsi qu’ après 3-4 jours. A la suite du traitement, les valeurs d’ inflammation doivent diminuer normalement (7). En l’ absence d’ une diminution de la CRP (< 25-50 % de la valeur de référence) ou du PCT, l’ échec du traitement devrait être ciblé (8). Cependant, les paramètres de l’ inflammation doivent toujours être interprétés en tenant compte du tableau clinique et de l’ état du patient. S’ il y a des signes de dysfonctionnement d’ un organe, son fonctionnement doit être vérifié au cours de la maladie, habituellement en vérifiant les paramètres de laboratoire comme p. ex. créatinine, transaminases ou cholestase, lactate, BNP, troponine, électrolytes, etc..
Échographie de la plèvre
Chez les patients hospitalisés atteints d’ une PAC avec épanchement pleural, un suivi échographique doit être effectué pour détecter le développement d’ un épanchement compliqué ou d’ un empyème pleural. Si une telle suspicion existe, une ponction pleurale diagnostique doit être effectuée.
Examen radiologique
Une radiographie pulmonaire de suivi n’ est pas systématiquement indiquée s’ il y a une réponse clinique adéquate au traitement. Chez les patients ayant des facteurs de risque pour une maladie tumorale, chez les fumeurs actifs, les anciens fumeurs, chez les patients de plus de 65 ans ou des patients atteints de maladies concomitantes graves, une tomodensitométrie doit être effectuée pour exclure une tumeur ou des infiltrats pulmonaires non infectieux. Chez les patients plus âgés ayant des antécédents de tabagisme, il y a un risque accru de cancer du poumon, qui peut soit imiter la pneumonie, soit causer une pneumonie poststenotique. Chez les patients ≥ 65 années, une malignité pulmonaire nouvellement diagnostiquée est trouvée au cours d’ une moyenne de moins d’ un an avec une incidence de 9, 2 %, et seulement 27 % de ce nombre dans les 90 jours suivant la sortie de l’ hôpital (9). La normalisation de l’ image radiographique du thorax peut durer des semaines, voire des mois. Par conséquent, si le patient répond cliniquement, une radiographie thoracique de contrôle doit être effectuée au plus tôt 2 semaines après la fin de l’ antibiothérapie.
L’ auteur n’ a déclaré aucun conflit d’ intérêts en rapport avec cet article.
La PAC représente une létalité non-négligeable, en particulier chez les personnes âgées de plus de 65 ans présentant une polymorbidité
Les investigations et le traitement sont basés sur l’ âge, l’ état général, les paramètres cliniques, la comorbidité ainsi que le spectre des pathogènes attendus
L’ indice CRB-65 permet une évaluation des risques et aide à décider si un traitement ambulatoire ou hospitalier est approprié
L’ élucidation des diagnostics différentiels et la détection précoce des complications potentielles d’ une pneumonie sont importantes.
La flore alpine est l’ une des plus fascinantes et compte une grande diversité d’ espèces. Les fleurs, souvent de couleurs intenses et très lumineuses, ne nous laissent pas indifférents : elles nous attirent par leur beauté.
Les plantes des Alpes poussent dans des conditions climatiques extrêmes selon l’ altitude : grands froids avec sols gelés pendant plusieurs mois, neige, vents violents et exposition à une lumière UV très intense. Elles ont su s’ adapter à ces conditions en synthétisant des constituants pour se protéger. Par exemple, ces espèces contiennent beaucoup d’ antioxydants et des capteurs de radicaux libres pour résister à la radiation UV intense. Ces substances peuvent aussi servir à l’ homme. Ainsi, par exemple, l’ edelweiss riche en antioxydants sert à la préparation de produits cosmétiques et dermatologiques pour ralentir le vieillissement de la peau.
Dans le présent ouvrage, les principales plantes des Alpes utilisées en médecine traditionnelle ou ayant conduits déjà à des médicaments enregistrés, sont présentées par leurs aspects botaniques, phytochimiques et pharmacologiques. Des conseils pratiques sont donnés afin de ne pas les confondre avec d’ autres espèces toxiques ou non toxiques. Il faut aussi savoir les utiliser correctement pour traiter une pathologie donnée, soit en usage interne ou externe. Des recettes pour préparer des tisanes, décoctions, huiles, teintures-mères et autres seront expliquées avec leurs modes d’ utilisations. Des effets secondaires éventuels ou des interractions avec d’ autres médicaments seront indiqués.
Les plantes bénéfiques pour la santé sont nombreuses. Cependant, les Alpes recèlent aussi passablement d’ espèces toxiques qui causent surtout des troubles gastro-intestinaux et autres désagréments, mais un nombre restreint de plantes peuvent induire une intoxication mortelle ! Gare aux pièges : les très belles plantes sont souvent les plus dangereuses ! L’ anonit de Napel avec ses superbes fleurs bleues en forme de casque de Jupiter peut conduire à la mort ! Mais, en très faibles doses (homéopathie, spagyrie), elle devient un médicament pour lutter contre les troubles circulatoires. Les principales plantes toxiques des Alpes sont décrites avec des indications pour les reconnaître facilement. Les circonstances d’ une intoxication, les symptômes, les mesures à prendre et les premiers secours seront clairement indiqués.
Ce guide pratique, illustré par des photographies en couleur, s’ adresse au grand public et aussi aux professionnels de la santé. Un outil utile pour toutes les personnes désireuses de connaître les plantes qu’ elles rencontrent lors de promenades et d’ excursions dans le massif alpin.
Luo YH et al. 5-year overall survival in patients with lung cancer eligible or ineligible for screening according to US Preventive Services Task Force criteria: a prospective, observational cohort study. Lancet Oncol 2019; 26: June 26, 2019 http://dx.doi.org /10.1016/ S1470-2045
The National Lung Screening Trial (NLST) randomisierte Patienten mit hohem Lungenkrebsrisiko (55- 74j., aktive Raucher mit > 30 pack years, oder ehemalige Raucher, die vor < 15 Jahren mit dem Rauchen aufgehört hatten) in eine Gruppe mit regelmässigen Thorax-Röntgenbildern (deren «Unwirksamkeit» für diesen Zweck bereits bekannt war) und eine zweite Gruppe mit regelmässigem Thorax-CT Screening (NEJM 2011; 365: 395). Die Studie suggerierte, dass CT Screening eine relative Mortalitätssenkung an Lungenkrebs von 20% erziele. Die Interpretation der Daten ergab (nicht zum ersten Mal in der medizinischen Fachliteratur) eine transatlantische Differenz. Die American Cancer Society war beeindruckt und empfahl den Risikopersonen ein Lungenkarzinom CT-Screening (trotz der vielen falsch positiven Befunde) (CA CANCER J CLIN 2017;67:100–121).
Die Verfasser der deutschen S3 Leitlinie und die Schweizerische Lungenliga waren nicht beeindruckt, und sie empfehlen bis auf den heutigen Tag kein Routine CT-Screening bei schweren Rauchern.
Und jetzt diese Studie, aufgrund der die US Preventive Services Task Force nun CT Screening sogar bei Patienten empfiehlt, die vor mehr als 15 Jahren mit dem Rauchen aufgehört hatten, oder die jünger sind als die Patienten in der NLST Studie. Die Studie zeigt einen ganz anderen Aufbau, und deshalb klare Schwächen im Vergleich zum NLST. Sie ist eine reine Beobachtungsstudie, die Patienten aufnahm, bei denen bereits ein Lungenkarzinom diagnostiziert worden war (nicht etwa Risikopersonen wie in der NLST) mit Charakteristika (Alter, Rauchergewohnheiten), die jedoch die Einschlusskriterien der NLST ausweiteten. Die eine Kohorte setzte sich aus hospitalisierten Lungenkarzinom-Patienten der Mayo-Klinik, Rochester, zusammen, die andere Patientenkohorte war eine Community Cohort aus Olmsted County (beide aus dem US-Bundesstaat Minnesota, Land of 10 000 Lakes, bisher in den Händen der Demokraten, aber ein potentieller «swing State» für die Präsidentschaftswahlen im Jahre 2020 – so watch it guys, and just behave yourselves, will ye!). Die Studie fand, dass die Lungenkrebs-Patienten, die für das NLST nicht qualifiziert hätten, dennoch eine vergleichbare (vergleichbar schlechte) Prognose hatten wie die NLST Studienpatienten. Leider wird, nicht klar, wie viele dieser rauchenden Minnesotans ihre Karzinom-Diagnose via CT Screening erhalten hatten.
Die Schlussfolgerung, auch diesen Risikopatienten müsse ein Lungenkarzinom CT Screening angeboten werden, scheint mir etwas abenteuerlich. Die vorliegende Studie prüfte den Wert der Frühdiagnostik von Lungenkarzinom nicht im mindesten. Logischerweise müsste das NLST mit diesen erweiterten Einschlusskriterien wiederholt werden, bevor ausgeweitete Empfehlungen vorgelegt werden können. Eine neue grosse randomisierte Studie ist allerdings Wunschdenken. Wenn aus europäischer Sicht Risikopersonen, die der NLST-Population entsprechen, nicht zwingend ein CT Screening erhalten sollen, dann gilt das erst recht für die ausgeweitete Population der vorliegenden Kohorten-Studie.
Es ist in summa wohl besser, schlicht und einfach nicht zu rauchen, und zu diesem Thema politische Signale auszusenden. So hätte Bundesrat Dr. med. Ignazio Cassis (MPH!) von vorneherein gar nicht in Betracht ziehen sollen, den Schweizer Auftritt an der EXPO 2020 in Dubai durch die Tabakindustrie zu Reklamezwecken finanzieren zu lassen.
Bevacizumab bei Ovarial- und Mammakarzinom
Tewari KS et al. Final overall survival of a randomized trial of bevacizumab for primary treatment of ovarian cancer. J Clin Oncol 2019; 37: DOI https://doi. org/10.1200/JCO.19. 01009.
Zusammenfassung: GOG-0218 untersuchte bei Frauen mit Ovarialkarzinom (Stadien III und IV) Chemotherapie alleine, Chemotherapie zuzüglich Bevacizumab, und die Kombination zuzüglich Bevacizumab-Erhaltung. Die wichtigsten Schlussfolgerungen dieses Artikels, der die Daten der abschliessenden Studienanalyse vorlegt, sind (im copy paste aus dem Abstract gezogen): «No survival differences were observed for patients who received bevacizumab compared with chemotherapy alone. Disease-specific survival was not improved in any arm. No survival advantage was observed after censoring patients who received bevacizumab at crossover or as second line.» Das tönt sec und abschliessend negativ. Die Diskussion ist jedoch interessant und ausgewogen geschrieben, so dass ich statt einer Würdigung des Papiers aus meiner Feder lieber ein paar allgemeine persönliche Bemerkungen zum Stellenwert von Bevacizumab formuliere.
Pivot X et al. 6 months versus 12 months of adjuvant trastuzumab in early breast cancer (PHARE): final analysis of a multicentre, open-label, phase 3 randomised trial. Lancet 2019; 393: 2591–98
Earl HM et al: 6 versus 12 months of adjuvant trastuzumab for HER2-positive early breast cancer (PERSEPHONE): 4-year disease-free survival results of a randomised phase 3 non-inferiority trial. Lancet 2019; 393: 2599–612
Zusammenfassung: Zwei Studien, praktisch gleich aufgegleist, im selben LANCET-Heft publiziert, und doch mit diametral verschiedenen Schlussfolgerungen. Sowohl die französische (PHARE) als auch die britische Studiengruppe (PERSEPHONE) fragten, ob bei der adjuvanten Therapie des HER2 POS Mammakarzinoms eine Behandlung mit nur 6 Monaten Trastuzumab nicht wirklich schlechter wäre als die Therapie mit der heutigen Standarddauer von 12 Monaten. Die frankophone PHARE Studie folgert, 12 Monate Verabreichungsdauer des Antikörpers bleibe Standard, die anglophile PERSEPHONE Studie kommt genau zum gegenteiligen Schluss. Wer hat Recht? La haute cuisine des essais cliniques de France (PHARE), oder Fish & Chips (PERSEPHONE)? L’Élysée, oder 10 Downing Street?
Milchprodukte, Prostata- und Blasenkarzimon
Preble I et al. Dairy Product Consumption and Prostate Cancer Risk in the United States. Nutrients 2019; 11: 161. doi:10.3390/nu11071615
Acham M et al. Intake of milk and other dairy products and the risk of bladder cancer: a pooled analysis of 13 cohort studies. Eur J Clin Nutr 2019; https://doi.org/10.1038/s41430-019-0453-6.
Vasconcelos A, et al. Dairy Products: Is there an impact on promotion of prostate cancer? A Review of the Literature. Front. Nutr. 2019; 6: 62. doi: 10.3389/fnut.2019.00062Aune D et al. Dairy products, calcium, and prostate cancer risk: a systematic review and meta-analysis of cohort studies.
Am J Clin Nutr. 2015; 101: 87-117. doi: 10.3945/ajcn.113.067157
Prof. em. Dr. med. Martin Fey
Bern
martin.fey@insel.ch
Beratungsmandat bei Nestlé Health Sciences, Epalinges. Aktien bei Novartis Roche und Johnson&Johnson.